CLINICAL DATA
A 12-year-old female white patient with a weight of 44 kg was referred to our service. At 5 years old she had presented with dyspnea, fever and anorexia and was hospitalized for congestive heart disease and diagnosed as having rheumatic disease. She was released from hospital using digoxin and benzathine penicillin, which she did not use correctly. Since then, the signs and symptoms worsened until she suffered from dyspnea at the slightest effort.
At admittance, she was in a good general state, eupneic at rest, acyanotic, hydrated and ruddy. Her thorax was asymmetrical with bulging of the left hemithorax, ictus cordis was palpable in the 5th intercostal space with deviation to the left. Pulmonary auscultation was symmetrical without adventitious sounds. Precordia evidenced a regular heart beat and normal sounds with a diastolic suction murmur of +++/6 at the accessory aorta with irradiation to the lower left sternal border. The liver was palpable at 2 cm from the right costal border. There were rapid and palpable pulses in the four limbs. The divergent pressure differential was measured at 140/20 mmHg.
ELECTROCARDIOGRAM
Sinusal rhythm was observed with a heart rate of 70 beats per minute. The QRS complex axis was +60º with a PR interval of 0.20s, QRS of 0.08s and QTc of 0.33s. A left atrial overload was evidenced by a biphasic P wave at V1 with a greater (plus minus) negative reflection. Left ventricular overload was evidenced by a large R wave at V6 and deep S at V1, with evidence of volumetric etiology, as there were no repolarization changes at precordial derivations.
RADIOGRAM
The cardiac area was increased with a cardiothoracic index of 0.67. Slight pulmonary vascular prominence was evidenced.
ECHOCARDIOGRAM
Situs solitus was seen at levocardia. The venoatrial, atrioventricular and ventriculoarterial connections were concordant. Thickening of the left atrioventricular (mitral) and aortic valves was evidenced as was significant regurgitation of the aortic valve and moderate regurgitation of the mitral and tricuspid valves. There was a significant increase in the size of the left ventricular cavity with the function preserved, a ÄD of 32% and an ejection fraction of 63%.
DIAGNOSIS
The definitive diagnosis was injury to the valve due to rheumatic disease requiring surgery as defined by the echocardiographic and Doppler images as well as the clinical state and complementary laboratorial examinations. A cineangiography was unnecessary.
OPERATION
Median transsternal thoracotomy was performed and cardiopulmonary bypass was established under hypothermia of 25ºC, using intermittent anterograde sanguineous cardioplegia at 4ºC directly to the coronary ostia. After opening the right atrium and interatrial septum lengthwise, plasty of the mitral valve was achieved using a nº 32 Gregori's ring [1], as shown in Figure 1. The aortic valve with its thickened cusps was retracted and without adequate mobility (Figure 2) it was resectioned and a nº 23 mechanical prosthesis was implanted in the normal manner. The tricuspid valve was treated using the De Vega annuloplasty [2]. The perfusion and myocardial ischemic times were 197 and 138 minutes respectively. The patient remained in the intensive care unit for four days due to left ventricular dysfunction. In this time she received intravenous diuretic and inotropic drugs. She was released from hospital on the 12th day after admission using warfarin, digital and diuretic agents. The post-operative echocardiograph demonstrated that the left ventricular function was preserved with a normal ejection fraction of 66%, the mechanical prosthesis functioned normally, no mitral or tricuspid regurgitation was evidenced and the patient was in functional class I (NYHA).
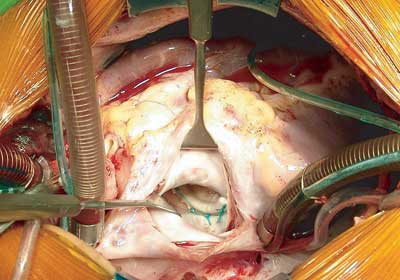
Fig. 1 - Gregori's ring utilized in the mitral valve plasty seen through the lengthwise opening in the interatrial septum
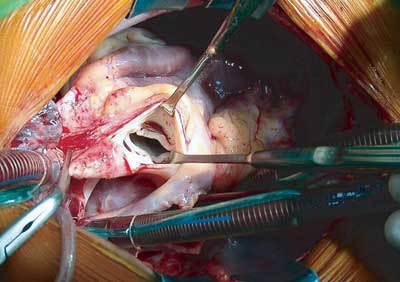
Fig. 2 - Aspect of the aortic valve affected by rheumatic disease
1. Gregori Jr F, Silva SS, Hayashi SS, Aquino W, Cordeiro C, Silva LR. Mitral valvuloplasty with a new prosthetic ring: Analysis of the first 105 cases. Eur J Cardiothorac Surg. 1994;8(4):168-72.
2. De Vega NG, De Rabago G, Castillon L, Moreno T, Azpitarte J. A new tricuspid repair: short-term clinical results in 23 cases. J Cardiovasc Surg. 1973;spec:384-6.
 All scientific articles published at rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at rbccv.org.br are licensed under a Creative Commons license













 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket