The authors report a clinical case of bird breeder who evolved with fever, myalgia, weight lost and negative blood cultures. On three occasions he was treated with different antibiotics, without improvement. He became progressively worse and after four months a diagnosis of endocarditis was made. An echocardiogram showed mitral valve dysfunction with vegetation that had not been seen previously. A blood test proved positive for Chlamydia psittaci (indirect immunofluorescence). In surgery the mitral valve was seen to have severe lesions with anterior cuspid rupture and large areas with vegetation. After surgery, he presented with a clinical improvement and was discharged on the thirteenth post-operative day on specific antibiotic therapy. Although rare, Chlamydia psittaci must be considered in cases of endocarditis with negative blood cultures, when there is a possibility of contact with birds.
Relatamos o caso de um criador de pássaros que desenvolveu um quadro consuntivo, febril, com mialgia e hemoculturas negativas. Internado por três ocasiões, foi tratado empiricamente com antibióticos, sem melhora. Após quatro meses, apresentou piora com sinais de infecção sistêmica. Ecocardiograma demonstrou insuficiência mitral moderada, com vegetações, não presentes em exame prévio. Sorologia positiva para Chlamydia psittaci (imunofluorescência indireta). Na cirurgia, identificou-se grande destruição da valva mitral, com cúspide anterior rota e vegetações. Após a cirurgia, apresentou melhora clínica, recebendo alta em treze dias, com antibioticoterapia específica. Apesar de pouco freqüente, a Chlamydia psittaci deve ser lembrada em casos de endocardite com hemoculturas negativas, quando houver história de exposição a pássaros.
INTRODUCTION
Infection endocarditis refers to bacterial or fungal infections inside the heart and diagnosis is suspected by the clinical signs and symptoms of the patient (fever, feeling bad, weight loss, fatigue, anorexia, nocturnal sudoresis, anemia, cutaneous or conjunctival petechiae, splenomegaly, among others). Diagnosis is confirmed by isolating the infecting microorganism in blood, an embolus or vegetation. Laboratorial confirmation of the infecting microorganism is particularly difficult and cultures can be negative in infections with fastidious microorganisms [1].
A review of publications identified few reports of endocarditis caused by Chlamydia psittaci [2,3]. We do not know if this number reflects the real incidence of endocarditis associated with Chlamydia psittaci or if many cases are not diagnosed due to the difficulty to identify the agent causing the infection.
Chlamydias are gram-negative parasitic bacteria that are described as three species: Chlamydia pneumoniae, Chlamydia trachomatis and Chlamydia psittaci [4]. Chlamydia psittaci produces a variety of infections in birds and lower mammals; in humans it usually causes pneumonia acquired by the inhalation of particles infected by secretions of birds [1]. The association between contact with birds and the development of acquired valvulopathies has already been described in the literature [5]. Generally, the infection affects previously abnormal valves, however, there are reports of the involvement of normal valves [4] with the aortic valve being the most commonly involved [1,4]. The clinical course of the infection can be acute or subacute-chronic based on the time of evolution, severity of the clinical presentation and on the progression of the non-treated disease [4,6].
In this report, we describe the case of a bird-breeder with prolapse of the mitral valve, who presented with mitral valve endocarditis and negative blood cultures. The serum and indirect immunofluorescence tests were positive for Chlamydia psittaci.
CASE REPORT
A 62-year-old lean Caucasian male patient, who was a bird salesman, in September 2002 presented with generalized muscle pain, fever (39 ºC) and indisposition. A blood test did not identify signs of infection; the partial urine test and chest and face sinus radiograms were normal. The HSV was 8 mm in the first hour. An investigation of salmonella was also negative. The administration of oral cephalexin was initiated. Ten days later, the patient was hospitalized for two days when he presented with anemia (hemoglobin = 11.60 g/dL) and a leukocyte count of 13,800 /mm3. A test for toxoplasmosis was negative. He was released from hospital taking 250 mg ciprofloxacin every 12 hours. Fifteen days later he was again hospitalized with fever, joint pain and weight loss. The anemia had worsened (hemoglobin = 11.40 g/dL) and the leukocyte count was 11,000 /mm3. An echocardiogram demonstrated a dense mitral valve with prolapse of the posterior cuspid and slight to moderate insufficiency without the presence of vegetation. Investigations of hematozoa, lsteriosis, anti-HIV antibodies and three blood cultures were all negative. BAAR was negative in sputum. Testing with tuberculostatic therapy was initiated.
In January 2003, the patient was again hospitalized with myalgia, artralgia, irritating cough, deterioration of the general health, weight loss and anorexia. Lung auscultation demonstrated crackles at the right base and heart auscultation evidenced systolic murmur at a mitral focus +/6. The hemoglobin was 10.6 g/dL, leukocytes 12,400/mm3 and HSV = 35 mm in the first hour. A test for Chlamydia psittaci antibodies was requested. A control echocardiogram demonstrated the right atrium slightly enlarged, the left ventricle dilated with normal function, the mitral valve dense, prolapse of the posterior cuspid, the anterior cuspid with a mass of 2.2 x 1.7 cm with moving echo on the ventricular face and another pedicled on the atrial face with moderate mitral insufficiency. Administration of crystalline penicillin was initiated at 18,000,000 U/day associated with 240 mg gentamicin endovenously/day, 200 mg oral doxicyclin per day and 500 mg levofloxacin endovenously/day.
After ten days the patient continued with fever with new blood cultures negative. Another echocardiogram demonstrated an increase in the mitral valve reflux and so surgical treatment was indicated.
On January 17 2003 surgery was performed using median sternotomy, cardiopulmonary bypass, and moderate hypothermia. The ascending aorta and both vena cavae were cannulated and myocardial protection was achieved with normothermic anterograde sanguineous cardioplegia repeated at twenty-minute intervals. After left atriotomy, the insufficient mitral valve was exposed with the anterior cuspid ruptured and with vegetation of 2 x 2 cm (Figure 1).
The mitral valve was resected and a porcine prosthesis was implanted. After normalization of the body temperature, removal of the air from the left chambers, aortic declamping and return of the normal heartbeats the cardiopulmonary bypass was discontinued and the arterial and venous cannulae removed.
The patient evolved well postoperatively and was released from the ICU on the 2nd postoperative day. He remained afebrile on endovenous antibiotics for another 13 days when he was released from hospital on 200 mg doxicycline and 400 mg moxifloxacin daily.
Indirect immunofluorescence was reactive for psittacosis (tit. 1/80) and the anatomopathologic examination demonstrated histiocytary cells with multiple vacuolized cytoplasms and intravacuolar corpuscles (Figure 2), a finding consistent with morphologic characteristics identified in cases of infection by Chlamydia sp., which was confirmed by a specific immunohistochemical examination and by ultra-structural evaluation by electronic microscope.

Fig. 1 - Anterior cuspid of the mitral valve with vegetation
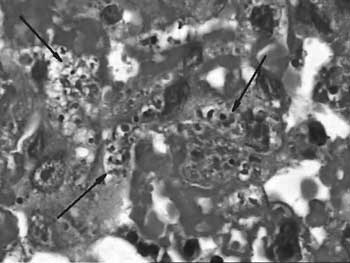
Fig. 2 - Histiocytary cells with multiple vacuolized cytoplasms and intravacuolar corpuscles (H&E - 1000x)
This report describes the case of a patient with mitral valve endocarditis caused by Chlamydia psittaci. The diagnosis, in this case was based on the clinical presentation, by the contact with birds, by serum positivity (reactive indirect immunofluorescence), by anatomopathologic examination, specific immunohistochemical examination and by ultra-structural evaluation using electronic microscopy of the mitral vegetation. The blood cultures were all negative.
As a predisposing factor, the patient presented with mitral valve prolapse, which is today, in industrialized countries, the most common cardiovascular lesion associated with mitral valve endocarditis, a greater indication of the high incidence of this lesion in the general population than the hemodynamic disorder caused by the valvar lesion [6], which is the highest risk in over 45-year-old men [7]. In developing countries injury caused by rheumatic fever is still the main predisposing factor of endocarditis.
Chlamydias are common human pathogens responsible for a wide range of infections including infections of the genitals, intestines, conjunctivitis and atypical pneumonias. In the heart, although infrequent, Chlamydia psittaci can cause endocarditis, myocarditis or pericarditis with negative blood cultures [4].
Endocarditis with negative blood cultures are responsible for 5% of the cases of endocarditis in native valves in this age range of patients (over 60-year-olds), and the commonly involved germs include, species of Bartonella, Coxiella burnetti, bacteria of the HACEK group (haemophilus, actinobacillus, cardiobacterium, eikella, kingella), Tropheryma whipplei, species of Legionella, species of Brucella and fungi [6] in addition to Chlamydia psittaci.
In spite of being difficult, diagnosis has important therapeutic implications in choosing the antibiotic therapy. Penicillin and other beta-lactamic antibiotics present little activity against Chlamydia and the aminoglycosides do not exert any therapeutic effect whatsoever. On the other hand, other antibiotics, such as tetracycline, doxicycline, fluoroquinolone, chloramphenicol, erythromycin and rifampin are efficacious [1,4,8].
Thus, it is necessary with patients with endocarditis and negative blood cultures, to identify the microorganism responsible and utilize an antibiotic therapeutic regimen at an effective dose. In cases of contact with birds or domestic animals such as cats [9], it is important to remember Chlamydia psittaci and perform serologic and immunofluorescence tests for anti-Chlamydia antibodies.
Surgical indication should be considered early specifically if there are signs of progressive heart failure, embolic phenomenons, failure in etiologic treatment, the presence of perivalvar destruction (abscesses) or involvement of valvar prostheses [6,10]. This infection is highly destructive, the mortality rate is high and, in many cases, valve replacement is necessary [1,4,11]. The use of antibiotics should be prolonged for at least thirty days after the surgical treatment, although the ideal time is still not known [4,8].
ACKNOWLEDGMENT
To professor assistant-PHD of Unifesp/EPM, Doctor Luiz A. R. Moura, responsible by the area os Renal Pathology of Fundação Oswaldo Ramos - Hospital do Rim e Hipertensão, by microscopic optical image.
REFERENCES
1. Jones RB, Priest JB, Kuo C. Subacute chlamydial endocarditis. JAMA.1982;247(5):655-8.
2. Shapiro DS, Kenney SC, Johnson M, Davis CH, Knight ST, Wyrick PB. Brief report: Chlamydia psittaci endocarditis diagnosed by blood culture. N Engl J Med. 1992;326(18):1192-5.
3. Etienne J, Ory D, Thouvenot D, Eb F, Raoult D, Loire R et al. Chlamydial endocarditis: a report on ten cases. Eur Heart J. 1992,13(10):1422-6.
4. Odeh M, Oliven A. Chlamydial infections of the heart. Eur J Clin Microbiol Infect Dis. 1992;11(10):885-93.
5. Ward C, Ward AM. Acquired valvular heart-disease in patients who keep pet birds. Lancet. 1974;2(7883):734-6.
6. Mylonakis E, Calderwood SB. Infective endocarditis in adults. N Engl J Med. 2001;345(18):1318-30.
7. Zuppiroli A, Rinaldi M, Kramer-Fox R, Favilli S, Roman MJ, Devereux RB. Natural history of mitral valve prolapse. Am J Cardiol. 1995;75(15):1028-32.
8. Walker LJ, Adgey AA. Successful treatment by doxycycline of endocarditis caused by ornithosis. Br Heart J. 1987;57(1):58-60.
9. Regan RJ, Dathan JR, Treharne JD. Infective endocarditis with glomerulonephritis associated with cat chlamydia (Chlamydia psittaci) infection. Br Heart J. 1979;42(3):349-52.
10. Dias AR, Pomerantzeff PM, Brandão CMA, Dias RR, Grinberg M, Lahoz EV et al. Tratamento cirúrgico da endocardite infecciosa ativa: análise de 361 doentes operados. Rev Bras Cir Cardiovasc. 2003;18(2):172-7.
11. Lamaury I, Sotto A, Le Quellec A, Perez C, Boussagol B, Ciurana AJ. Chlamydia psittaci as a cause of lethal bacterial endocarditis. Clin Infect Dis. 1993;17(4):821-2.
 All scientific articles published at rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at rbccv.org.br are licensed under a Creative Commons license













 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket