![]()
![]()
Walter J GomesI; Raul E. SaavedraII; Débora M. GaranhãoIII; Alexandre R. CarvalhoIV; Francisco A. AlvesV
DOI: 10.5935/1678-9741.20110043
RESUMO
OBJETIVO: A cirurgia de reconstrução do ventrículo esquerdo (VE) é efetiva no tratamento da cardiomiopatia isquêmica com grandes áreas acinéticas ou discinéticas. Entretanto, resultados de sobrevida tardia estão relacionados ao tamanho da cavidade ventricular esquerda remanescente, portanto eliminar retalhos intracavitários pode proporcionar redução adicional do VE. O objetivo deste trabalho foi analisar os resultados com a cirurgia de reconstrução ventricular esquerda utilizando o conceito da máxima redução ventricular, com sistemática eliminação de retalhos.
MÉTODOS: Setenta e seis pacientes consecutivos com cardiomiopatia isquêmica (idade 30-78 anos, média 57,6 ± 10,1), evoluindo em classe funcional III e IV foram submetidos à cirurgia de reconstrução ventricular direta sem utilização de retalhos intracavitários ou materiais protéticos.
RESULTADOS: O diâmetro sistólico final do VE diminuiu de 52,3 ± 5,4 no pré-operatório para 45,2 ± 6,9 mm no pós-operatório. A fração de ejeção aumentou de 34,2% ± 10,4% para 45,5% ± 9,4%. Revascularização miocárdica associada foi realizada em 75/76 pacientes, com média de 2,4 enxertos/paciente. Mortalidade em 30 dias foi 3/76 (3,9%). No acompanhamento médio de 39 meses, a maioria dos pacientes (91,4%) permanece em CF I ou II.
CONCLUSÃO: O conceito de maximizar a redução do VE com a reconstrução sistemática sem uso de retalhos mostrou-se viável, segura e eficaz, com os resultados precoces e tardios comparando favoravelmente às séries relatadas na literatura médica. Além disso, o conceito harmoniza-se à base fisiopatológica contemporânea da insuficiência cardíaca.
ABSTRACT
OBJECTIVES: The reconstruction of the left ventricle (LV) is effective in the treatment of ischemic cardiomyopathy with large akinetic or dyskinetic areas. However, late survival outcomes are related to the remnant left ventricular cavity size, thus eliminating intracavitary patch placement provides additional LV reduction. The aim of this study was to analyze the results with left ventricular reconstruction surgery using the concept of maximum ventricular reduction, with systematic patch abolition.
METHODS: Seventy-six consecutive patients with ischemic heart disease (age 30-78 years, mean 57.6 ± 10.1), evolving in functional class III and IV underwent surgical ventricular reconstruction with no use of intracavitary patches or Teflon strips for closing the left ventriculotomy.
RESULTS: The left ventricular end-systolic diameter decreased from 52.3 ± 5.4 in the preoperative period to 45.2 ± 6.9 mm in the postoperative period. LV ejection fraction increased from 34.2% ± 10.4% to 45.5% ± 9.4%. Associated CABG was performed in 75/76 patients with a mean of 2.4 grafts per patient. The 30-day mortality was 3/76 (3.9%). At an average follow up of 39 months, the majority of the patients (91.4%) remain in functional class I and II.
CONCLUSION: The concept of maximizing LV reduction with systematic patchless reconstruction is feasible, safe and effective, the early and late outcomes comparing favorably to previous series reported in the medical literature. Additionally, the concept meets the contemporary pathophysiologic basis of heart failure.
INTRODUCTION
Surgical ventricular reconstruction (SVR) for treatment of ischemic cardiomyopathy has been demonstrated to significantly improve left ventricular function and quality of life, with symptom relief and functional class improvement in patients with heart failure.
The grounds for SVR were developed in the mid-1980s [1,2] and later modified by the RESTORE group [3], the aim of the procedure being to reduce size and reshape the left ventricular cavity with placement of a intraventricular patch. However, significant new evidences have been added over the last decades on the knowledge of pathophysiology and progression of heart failure; and its operative treatment. Recent evidence demonstrated that survival of patients evolving with heart failure and also after SVR is inversely correlated to the size of the residual left ventricular (LV) cavity, i.e., the final systolic and diastolic volumes [3].
Heart failure and myocardial ischemia have currently been recognized as disorders whose genesis and progression are related to inflammatory mechanisms and neurohormonal activation [4]. Also, the implant of prosthetic materials is documented to elicit and sustain a myocardial chronic inflammatory reaction, with ongoing release of inflammatory mediators. Therefore, eliminating the patch placement during LV reconstruction could contribute to further LV cavity reduction, virtual elimination of superimposed akinetic areas and potentially blunt myocardial chronic inflammatory reaction.
The aim of this study is to report the application and outcomes of these concepts in a large series of patients subjected to a more physiological approach in LV reconstruction; with systematic intracavitary patch elimination and avoidance of prosthetic material for LV closure.
METHODS
Patients
Between September 2002 and February 2008, 76 consecutive patients with ischemic cardiomyopathy and LV aneurysm (73 anterior wall and 3 inferior wall) underwent surgical LV reconstruction using the patchless technique described herein, at the Pirajussara General Hospital and Luzia de Pinho Melo Clinics Hospital. Both institutions are university-affiliated community hospitals serving lower-income population regions in the outskirts of Sao Paulo metropolitan area. All patients were referred for operation due to uncontrollable heart failure symptoms and/or refractory angina pectoris, despite optimized evidence-based medication. Preoperative assessment included coronary cineangiography with left ventriculogram and transthoracic echocardiography.
The patients age ranged from 30 to 78 years-old, with a mean of 57.6 ± 10.1 years. All operations were performed by a single surgeon and multiple assistants. The patients were followed until May 2008 and clinical follow-up was obtained via chart review, telephone interview and/or referring physician contact. The study protocol was approved by the institutional Ethics Committee.
Technique
Standard cardiac anesthesia was employed and Swan-Ganz catheter was not routinely inserted. Cardiopulmonary bypass (CPB) was established with a single two-stage cannula in the right atrium and ascending aorta cannulation, a vent was inserted through the right superior pulmonary vein and advanced across the left atrium and mitral valve into the left ventricle.
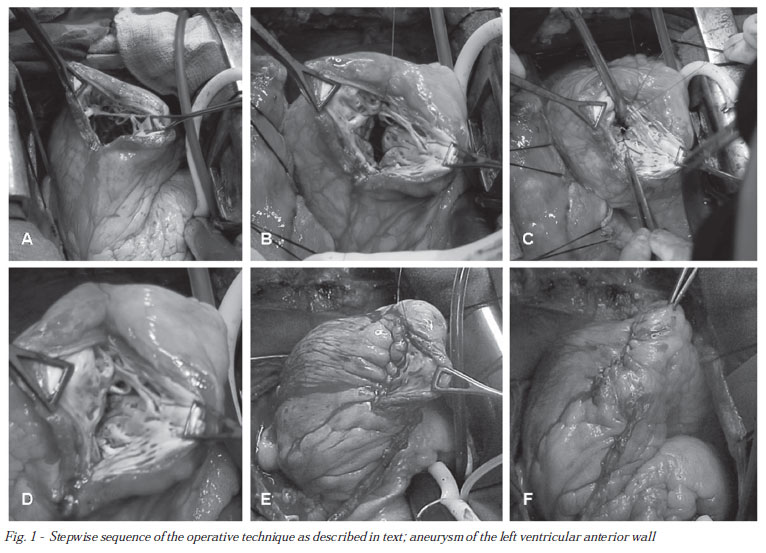
The procedure was carried-out with the empty beating heart technique without aortic cross-clamping, the coronary arteries perfused by orthograde flow from the aorta sustained by normothermic cardiopulmonary bypass. Perfusion pressure was kept above 80 mmHg throughout and patient continuously rewarmed to 36.5ºC. In cases of anterior wall aneurysm, the left ventricle anterior wall was carefully and sparingly incised at the aneurysmal area, parallel and at least 1.5 cm away from the interventricular septum and the left anterior descending (LAD) coronary artery, aiming to preserve both LAD and large diagonal arteries for subsequent grafting. Upon opening, LV cavity was carefully inspected and any existing thrombus entirely removed.
A double layer of 3-0 polypropylene purse-string sutures were placed around the aneurysm neck (the so-called Fontan stitch), i.e., at the level of transitional area between fibrotic tissue and healthy muscle, delimitated both in the septum and in the anterolateral wall, close to the anterolateral papillary muscle base. Next, the suture is tied down redefining the size of the remaining ventricular cavity and the edges of newly created orifice are brought together with a 3-0 polypropylene running suture. The edges of the remaining ventricular free wall were then closed using running and overlapping suture, with no use of Teflon felt strips or foreign material whatsoever (Figure 1).
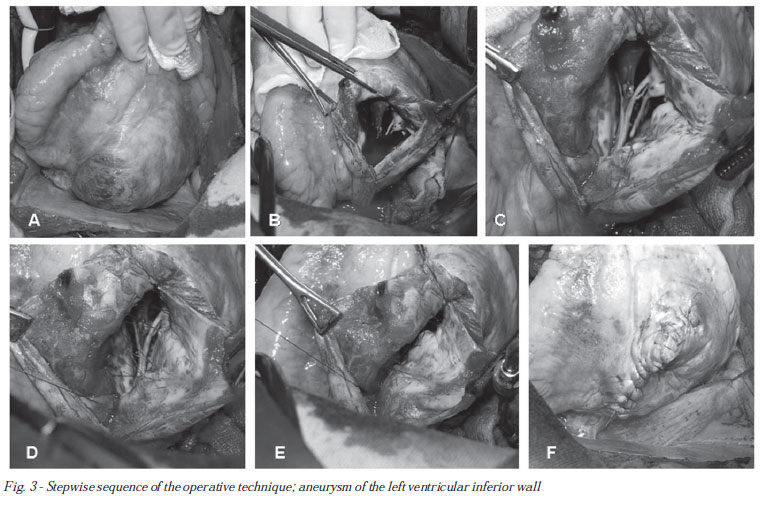
Great care is taken to avoid damage to diagonal branch and LAD, which are routinely revascularized using sequential LITA grafting whenever feasible (Figure 2). The distal coronary anastomoses are performed under pump-assisted circulation and with the aid of Octopus tissue stabilizer (Medtronic). The top-end anastomoses were completed using side-bite clamping. Similar technique was employed in case of inferior wall aneurysms, as can be seen is Figure 3.
Moderate to severe mitral valve regurgitation was considered an indication for mitral repair, performed in three patients by employing flexible rings.
In the latest one-third of this series, in eight patients a technical modification was implemented, with placement of the Fontan stich nearly one centimeter downwards the transitional zone, thereby overreducing the LV cavity.
RESULTS
Mean CPB time was 87.8 minutes, ranging from 35 to 150 minutes. Concomitant coronary artery bypass grafting was performed in 98.7% of the patients (75/76), with a mean of 2.4 grafts per patient. The left internal thoracic artery was grafted to the left anterior descending artery in 75/76 patients (98.7%). One patient with single-vessel disease was found to have the LAD totally fibrotic all way down, precluding further revascularization.
No patient required mechanical circulatory support with intra-aortic balloon pump (IABP) for CPB discontinuation or needed reoperation for bleeding. The median postoperative hospital stay was 6 days.
In roughly one quarter of patients (20 patients, 26.3%), CPB was discontinued with use of sodium nitroprusside only. The remainder required variable dose combinations of IV dobutamine, noradrenaline, nitroprusside, nitroglycerine, and metoprolol.
Overall 30-day mortality was 3.9% (3/76). Over the long-term follow-up, the left ventricular ejection fraction increased from 34.2% ± 10.4% preoperatively to 45.5% ± 9.4% postoperatively. The left ventricular end-systolic diameter decreased from 52.3 ± 5.4 in the preoperative period to 45.2 ± 6.9 mm in the postoperative period and the end-diastolic diameter from 65.0 ± 4.1 to 58.7 ± 5.8 mm. In the mean follow-up of 39 months, 5 patients died (survival at 39 months = 93.1%). Causes of late death included neoplasia (2 patients), chronic obstructive pulmonary disease complication (1), arrhythmia (1) and unknown (1). The majority of the patients in this series (91.4%) remain in functional class I or II after the operation. Postoperatively, all patients are on continued evidence-based medication for heart failure control using a combination of angiotensin-converting enzyme inhibitors, cardioselective beta-blockers, spironolactone, digoxin, and furosemide, which are provided free-of-charge or at subsidized cost by the local public health system.
DISCUSSION
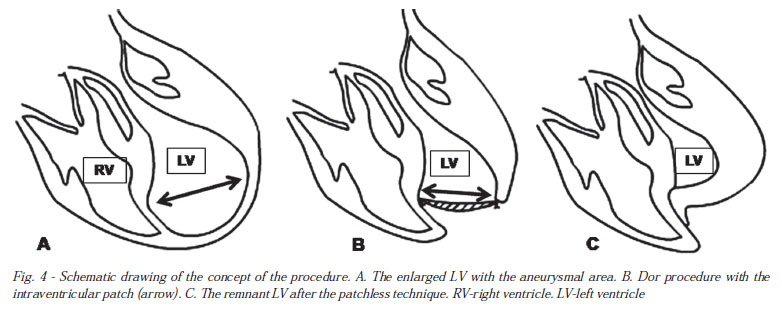
The present operative concept (Figure 4) and technique incorporate and merge much of recently acquired evidence on heart failure, its pathophysiology, mechanics and biochemical aspects. Our preliminary study reporting the satisfactory outcomes have encouraged us to proceed further in implementing the concept [5].
The size of the LV cavity has been unequivocally demonstrated correlate with survival in patients with heart failure [3,6]. The larger the size of the LV cavity, the lower the expected survival, thus LV dilation is an independent contributor to poor outcome in patients with advanced heart failure [7]. The ongoing progression of ventricular dilation leads to increased wall tension, according to the LaPlace's law and the attenuation or reversion of this process is linearly associated with improved systolic performance and reduced risk of further cardiovascular events [8,9].
In the SAVER study, the postoperative LV size was also a significant and decisive risk factor for late survival. Patients with postoperativeend-systolic volume index (ESVI) up to 80 ml/m2 had higher survival at 3 years compared with those with ESVI > 80 ml/m2. strengthening that elimination of LV akinetic areas, as well as diskinetic areas could potentially lead to better restoration of LV function [8]. For accomplishment of this goal, virtual exclusion of non-contractile and non-viable myocardial areas (scar) seems imperative for left ventricular function improvement.
The STICH trial, set to study the impact of revascularization plus SVR versus revascularization only in the treatment of severe ischemic cardiomyopathy, concluded that adding SVR to CABG was not associated with a greater improvement in symptoms, exercise tolerance or reduced immediate mortality. This disappointing finding has largely been ascribed to an inadequate SVR procedure with insufficient LV volume reduction, with an average end-ESVI reduction of 19% only, compared to a figure of 40% reported by the SAVER study [10].
Although studies demonstrate that current employed techniques of ventricular reconstruction (included Dor procedure and the variant SVR - Surgical Ventricular Restoration) improve global LV systolic function, the mechanism and effect on regional LV systolic function remains poorly understood [11]. While patch (geometric) left ventricular reconstruction suggest provide favorable results, meta-analysis comparing early outcomes following geometric versus linear reconstruction found no difference between the two surgical approaches when performed in the same time span, with similar in-hospital mortality and other end-points (postoperative inotrope requirement, low output syndrome, and need of intra-aortic balloon pump) [12]. Additionally, the 10-year survival rate showed no significant difference between the linear resection and patch ventriculoplasty groups [11,13].
On the other hand, numerous evidences demonstrated that inflammation plays an important role in the development and progression of heart failure. Heart failure is now recognized as a syndrome characterized by prolonged immune and inflammatory activation, with high circulating levels of pro-inflammatory cytokines and an increased expression of several other inflammatory mediators. These inflammatory mediators are not only markers of immune activation, but also induce myocardial dysfunction by different mechanisms, including the regulation of apoptosis, the beta-adrenergic responsiveness, and adverse remodeling [14]. Studies to date have suggested that elevated circulating levels of pro-inflammatory cytokines are associated with increased mortality [15]. Likewise, coronary artery disease and LV ischemic dysfunction is also characterized by immune inflammatory activation and inflammatory mediators have a major role in the development and progression of arteriosclerosis 16].
Following LV aneurysm formation and consequent expansion of LV chamber, neurohormonal system activation (brain natriuretric peptide - BNP, norepinephrine, renin and angiotensin II) take place and its concentrations are associated to worse prognosis and also predict long-term survival. The SVR, resulting in reduction of chamber dimensions and decrease in the ventricular filling pressures and wall tension, is accompanied by improvement of the neurohormonal response [17].
Prosthetic material customarily employed in LV reconstruction (Dacron patch, Teflon felt and bovine pericardium) are recognized to elicit a foreign body reaction with a consequent myocardial chronic inflammatory response. Previous studies showed that Teflon and bovine pericardium are associated with predominantly mononuclear inflammatory infiltrate (monocytes and macrophages) in the adjacent tissue and induction of a graft-versus-host immunological response. These formations constitute an active source of cytokines (interleukins and tumor necrosis factor), which trigger and sustain inflammatory processes induced by foreign substances in the organism over the long-term [5-18].
A further consequence of the chronic myocardial inflammatory reaction induced by foreign materials is an exuberant scar formation around the prosthetic material and infiltrating the surrounding cardiac muscle. Extensive myocardial scar tissue and severely depressed left ventricular ejection fraction (LVEF) are independent predictors of death or recurrent ventricular arrhythmias in patients with coronary artery disease [19]. Sudden death is the most common single mode of death during long-term follow-up after left ventricular reconstruction, this high incidence of late sudden death is significantly associated to ventricular tachyarrhythmias [20].
Additionally, proinflammatory cytokines such as tumor necrosis factor (TNF), interleukin-1, and interleukin-6 are synthesized not only by cells of the immune system but also by cardiac myocytes in response to ischemia or mechanical stretch, promoting decreased cardiac contractility, interstitial fibrosis and collagen deposition in noninfarct zones and deleterious effects in the heart over time. Excessive scar formation critically diminishes myocardial compliance, which contributes to diastolic and eventually systolic dysfunction, disrupts myocyte-to-myocyte electrical connectivity, and further exacerbates the cycle of ischemic stress-inflammation-stress. Sustained expression of proinflammatory cytokines can extend to involve remote, noninfarcted regions and contribute to remodeling of the entire myocardium. [15,16,21].
The technique herein reported abolishes the use of intracavitary patch, excluding and virtually eliminating LV septal and free wall akinetic/dyskinetic areas, maximizing left ventricular cavity reduction and leaving only contractile myocardial segments. This concept complies directly with Laplaces law, where the maximized reduction of the left ventricular cavity diminishes the left ventricular wall tension, reducing oxygen consumption. Patch placement has also been demonstrated reduce overall LV compliance, as a consequence of use of a non-compliant material rather than excluding non-viable but still more compliant myocardium [21].
The beating heart technique employed in this series might have played a decisive role for the attained outcome and every step of the procedure (LV reconstruction, CABG and mitral repair) could be accomplished without aortic cross-clamping and cardioplegic arrest. Beating heart surgery has been demonstrated afford enhanced left ventricular function and to reduce troponin and CK-MB (markers of myocardial tissue damage) release compared to on-pump technique with aortic cross-clamping by eliminating intraoperative global myocardial ischemia, with preservation of native coronary blood flow, reduction of myocardial injury and inflammatory response, and thus contributing to myocardial protection [22,23]. In patients with depressed LV function, preservation of every cardiomyocyte counts and aortic cross-clamping induction of troponin and CK-MB release is a translation of further cell loss. Strong previous off-pump coronary bypass surgery experience in our center certainly contributed for mastering the beating heart technique [24]. Remarkably, even operating on patients with advanced left ventricular dysfunction, mechanical circulatory support with IABP has not been utilized in any case.
Additionally, in this technique the distance between mitral papillary muscles and between papillary muscles and leaflet free edge is shortened, affording reduction of the tethering mechanism with better cusp coaptation and mitral regurgitation improvement.
Associated coronary revascularization is essential in SVR, contributing to further clinical improvement. Grafting of the left anterior descending artery, even when totally occluded, is particularly important to provide blood flow for viable areas of the interventricular septum, serving as a source of collateral circulation for other myocardial segments and for control of ventricular arrhythmias originating from the transitional region. As in this technique a vessel-sparing ventricular incision is performed, complete revascularization of the coronary arteries in the anterolateral wall is easily accomplished.
Unlike Batista operation [25], which proposed LV reduction by mandatory excision of the inter-papillary lateral wall, this procedure excludes only scarred non-contractile segments, but following the same commandments.
The introduction of new cardiac imaging methods such as MRI and enhanced software might greatly contribute to this field, targeting more accurate delimitation of LV non-contractile and non-viable areas, providing more information leading to a greater precision in the cavity reconstruction and with potential to improve performance.
A limitation of the study resides in its historical prospective design and performed in multiple centers with limited imaging resources; this negatively affected our ability to obtain complete preoperative and postoperative cardiac volumetric measurements for all patients. Additionally, our study was not protocol driven, and patient care was determined by clinical judgment. Further prospectives trials with appropriate design should be able to define the role of the concept in the management of ischemic cardiomyophaty.
Finally, SVR is performed aiming to improve quality of life and possibly to extend survival. In this way, this technique has been proved to be not harmful and capable to afford to patients early and late outcomes comparing favorably to previous reported series.
CONCLUSION
Based on these results, the concept of maximizing LV reduction with systematic patchless reconstruction is feasible, safe and effective. Additionally, the concept meets contemporary pathophysiologic basis of heart failure.
REFERÊNCIAS
1. Dor V, Saab M, Coste P, Kornaszewska M, Montiglio F. Left ventricular aneurysm: a new surgical approach. Thorac Cardiovasc Surg. 1989;37(1):11-9. [MedLine]
2. Jatene AD. Left ventricular aneurysmectomy: resection or reconstruction. J Thorac Cardiovasc Surg. 1985;89(3):321-31. [MedLine]
3. Athanasuleas CL, Stanley AW, Buckberg GD, Dor V, Di Donato M, Siler W, et al. Surgical anterior ventricular endocardial restoration (SAVER) for dilated ischemic cardiomyopathy. Semin Thorac Cardiovasc Surg. 2001;13(4):448-58. [MedLine]
4. Anker SD, von Haehling S. Inflammatory mediators in chronic heart failure: an overview. Heart. 2004;90(4):464-70. [MedLine]
5. Gomes WJ, Jaramillo JI, Asanuma F, Alves FA. Physiologic left ventricular reconstruction: the concept of maximum ventricular reduction and minimum inflammatory reaction. Rev Bras Cir Cardiovasc. 2004;19(4):353-7. Visualizar artigo
6. Burns RJ, Gibbons RJ, Yi Q, Roberts RS, Miller TD, Schaer GL, et al. The relationships of left ventricular ejection fraction, end-systolic volume index and infarct size to six-month mortality after hospital discharge following myocardial infarction treated by thrombolysis. J Am Coll Cardiol. 2002;39(1):30-6. [MedLine]
7. Vasan RS, Larson MG, Benjamin EJ, Evans JC, Levy D. Left ventricular dilatation and the risk of congestive heart failure in people without myocardial infarction. N Engl J Med. 1997;336(19):1350-5. [MedLine]
8. Athanasuleas CL, Buckberg GD, Stanley AW, Siler W, Dor V, Di Donato M, et al. Surgical ventricular restoration in the treatment of congestive heart failure due to post-infarction ventricular dilation. J Am Coll Cardiol. 2004;44(7):1439-45. [MedLine]
9. Walker JC, Guccione JM, Jiang Y, Zhang P, Wallace AW, Hsu EW, et al. Helical myofiber orientation after myocardial infarction and left ventricular surgical restoration in sheep. J Thorac Cardiovasc Surg. 2005;129(2):382-90. [MedLine]
10. Jones RH, Velazquez EJ, Michler RE, Sopko G, Oh JK, OConnor CM, et al. Coronary bypass surgery with or without surgical ventricular reconstruction. N Engl J Med. 2009;360(17):1705-17. [MedLine]
11. Antunes PE, Silva R, Ferrão de Oliveira J, Antunes MJ. Left ventricular aneurysms: early and long-term results of two types of repair. Eur J Cardiothorac Surg. 2005;27(2):210-5. [MedLine]
12. Parolari A, Naliato M, Loardi C, Denti P, Trezzi M, Zanobini M, et al. Surgery of left ventricular aneurysm: a meta-analysis of early outcomes following different reconstruction techniques. Ann Thorac Surg. 2007;83(6):2009-16. [MedLine]
13. Lange R, Guenther T, Augustin N, Noebauer C, Wottke M, Busch R, et al. Absent long-term benefit of patch versus linear reconstruction in left ventricular aneurysm surgery. Ann Thorac Surg. 2005;80(2):537-41
14. Devaux B, Scholz D, Hirche A, Klovekorn WP, Schaper J. Upregulation of cell adhesion molecules and the presence of low grade inflammation in human chronic heart failure. Eur Heart J. 1997;18(3):470-9. [MedLine]
15. Sun M, Chen M, Dawood F, Zurawska U, Li JY, Parker T, et al. Tumor necrosis factor-mediates cardiac remodeling and ventricular dysfunction after pressure overload state. Circulation. 2007;115(11):1398-407. [MedLine]
16. Aukrust P, Ueland T, Lien E, Bendtzen K, Muller F, Andreassen AK, et al. Cytokine network in congestive heart failure secondary to ischemic or idiopathic dilated cardiomyopathy. Am J Cardiol. 1999;83(3):376-82. [MedLine]
17. Schenk S, McCarthy PM, Starling RC, Hoercher KJ, Hail MD, Ootaki Y, et al. Neurohormonal response to left ventricular reconstruction surgery in ischemic cardiomyopathy. J Thorac Cardiovasc Surg. 2004;128(1):38-43. [MedLine]
18. Hernandez-Pando R, Bornstein QL, Aguilar Leon D, Orozco EH, Madrigal VK, Martinez Cordero E. Inflammatory cytokine production by immunological and foreign body multinucleated giant cells. Immunology. 2000;100(3):352-8. [MedLine]
19. van der Burg AE, Bax JJ, Boersma E, Pauwels EK, van der Wall EE, Schalij MJ. Impact of viability, ischemia, scar tissue, and revascularization on outcome after aborted sudden death. Circulation. 2003;108(16):1954-9. [MedLine]
20. Matthias Bechtel JF, Tölg R, Graf B, Richardt G, Noetzold A, Kraatz EG, et al. High incidence of sudden death late after anterior LV-aneurysm repair. Eur J Cardiothorac Surg. 2004;25(5):807-11. [MedLine]
21. Ueno T, Sakata R, Iguro Y, Yamamoto H, Ueno M, Ueno T, et al. Mid-term changes of left ventricular geometry and function after Dor, SAVE, and Overlapping procedures. Eur J Cardiothorac Surg. 2007;32(1):52-7. [MedLine]
22. Izumi Y, Magishi K, Ishikawa N, Kimura F. On-pump beating-heart coronary artery bypass grafting for acute myocardial infarction. Ann Thorac Surg. 2006;81(2):573-6. [MedLine]
23. Rastan AJ, Bittner HB, Gummert JF, Walther T, Schewick CV, Girdauskas E, et al., On-pump beating heart versus off-pump coronary artery bypass surgery - evidence of pump-induced myocardial injury. Eur J Cardiothorac Surg. 2005;27(6):1057-64. [MedLine]
24. Gomes WJ, Tavares GB, Jaramillo JI, Alves FA, Torrijos JMG, Catani R, et al. Off-pump grafting of the circumflex artery with pedicled retro-aortic right internal thoracic artery graft. Rev Bras Cir Cardiovasc. 2005;20(1):33-8. Visualizar artigo
25. Batista RJ, Santos JL, Takeshita N, Bocchino L, Lima PN, Cunha MA. Partial left ventriculectomy to improve left ventricular function in end-stage heart disease. J Card Surg. 1996;11(2):96-7.
Article receive on segunda-feira, 25 de julho de 2011
 All scientific articles published at rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at rbccv.org.br are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()
 Read in English
Read in English
 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}