![]()
![]()
Leonardo Secchin CanaleI; Alexandre Siciliano ColafranceschiII; Andrey José Oliveira MonteiroIII; Bruno Miranda MarquesIV; Clara Secchin CanaleV; Ernesto Chavez KoehlerIV; Fernando Eugênio dos Santos Cruz FilhoV
DOI: 10.5935/1678-9741.20110046
ABSTRACT
OBJECTIVE: To analyze the effectiveness of surgical treatment of atrial fibrillation (AF) using bipolar radiofrequency ablation during mitral valve procedures of rheumatic etiology in heart surgery.
METHODS: We retrospectively reviewed medical registries of 53 patients submitted to atrial ablation with bipolar radiofrequency energy during mitral valve surgery. Thirty four (64%) patients were women and the age varied from 27 to 72 years old (average: 49.3 ± 10.7 years). Aortic and/or tricuspid procedures were also present in 36 (68%) patients. Average time of reported atrial fibrillation was 41 months (from 3 to 192 months). Type of AF was classified as: paroxysmal in 8 patients, persistent in 3, permanent in 42. Left atrium had an average size of 52.9 ± 8.5 mm. The surgeries in these series were: 47 mitral valve replacements and 6 mitral valve repairs. Eletrocardiografic follow up was 83% complete in 14 months. Data from 24h Holter were explored.
RESULTS: Seven (13%) perioperative deaths were observed and survival after 14 months was 87%. Observed heart rhythm after 1 year of surgery was sinus rhythm in 25 (66%) patients, AF in 7 (18%), flutter in 7 (13%), junctional in 1 (3%).
CONCLUSION: Bipolar radiofrequency ablation in patients submitted to mitral valve surgery of rheumatic etiology is effective in converting to sinus rhythm in 68% of patients after 14 months.
RESUMO
OBJETIVO: Avaliar a eficácia do tratamento cirúrgico da fibrilação atrial (FA) utilizando ablação com radiofrequência bipolar durante cirurgia cardíaca de procedimentos mitrais de etiologia reumática.
MÉTODOS: Foram avaliados, retrospectivamente, os prontuários e exames de 53 pacientes submetidos à cirurgia valvar mitral, com ou sem cirurgia tricúspide ou aórtica associada, em que foi realizada ablação de FA utilizando radiofrequência bipolar. Trinta e quatro (64%) pacientes eram mulheres e a idade variou de 27 a 72 anos (média: 49,3 anos ± 10,7 anos). O tempo médio de FA relatado foi de 41 meses (variou de 3 a 192 meses). O tipo de FA apresentado foi: paroxística em oito pacientes, persistente em três, permanente em 42. O átrio esquerdo apresentava tamanho médio de 52,9 ± 8,5 mm. As cirurgias realizadas foram: 47 trocas de valva mitral e seis plastias mitrais. O seguimento eletrocardiográfico foi completo em 83% dos pacientes, ao final de 14 meses. Informações adicionais oriundas de Holter 24h foram exploradas.
RESULTADOS: Ocorreram sete (13%) óbitos per-operatórios e a sobrevida após 14 meses foi de 87%. Os ritmos cardíacos encontrados após um ano de cirurgia foram: sinusal em 25 (66%) pacientes, FA em sete (18%), Flutter em cinco (13%), Juncional em um (3%).
CONCLUSÃO: O uso de radiofrequência bipolar para tratamento de FA em pacientes submetidos à cirurgia valvar mitral de origem reumática é efetivo no controle da arritmia em 68% dos pacientes, após 14 meses.
INTRODUCTION
Atrial fibrillation (AF) may lead to significant morbidity and is associated with increased mortality [1]. While non-valvular AF is associated with increased risk of stroke two to seven times, AF associated with valvular disease increases this risk by 17 times [2]. Up to 10% of patients undergoing cardiac surgery and 45% of those undergoing surgical procedures for rheumatic mitral valve disease are associated with AF [3]. Surgical treatment of atrial fibrillation concomitant to the primary cardiac procedure is now widely accepted as safe and effective [4]. Despite the excellent results achieved when treating patients with degenerative mitral valve and other surgeries, AF associated with rheumatic mitral valve disease is less studied. The aim of this study is to report the mid-term clinical results and heart rate of patients undergoing bipolar radiofrequency ablation (RFB) concomitant with mitral valve surgery of rheumatic origin at National Institute of Cardiology, Rio de Janeiro.
METHODS
Between January 2008 and December 2009, 79 patients underwent AF ablation using RFB (AtriCure®) concomitant to major surgical procedure. Of this group, 53 patients underwent mitral valve surgery, associated ou not to tricuspid and aortic surgery due to rheumatic disease, and are the object of this study. Variables of interest were retrospectively collected according to guidelines on research in surgical treatment of AF [5]. We assessed the following variables: age, type of AF, AF time reported prior to surgery, prior ablative procedures, presence of pacemaker, cardiac diagnosis motivating the indication for surgery, left atrial size, left ventricular ejection fraction, a surgical procedure performed and set of injuries performed to treat AF.
Patients were followed postoperatively with clinic visits scheduled for 1, 3, 6 and 12 months postoperatively, and were assessed by a non-blind specialist to the treatment of AF, on the use of medications, cardiac rhythm, thromboembolic events, any percutaneous ablations in the postoperative period and reoperation. 24 three-channel Holter was requested from 6 months and assessed by a non-blind specialist to the treatment of AF. The therapeutic failure criterion used is of any tachyarrhythmia with a total duration greater than 24 in the 30s. In turn, the 24 hour Holter tests were assessed not only on the diagnosis of therapeutic failure, but also on other variables of interest: duration of the test, heart rate, minimum, average and maximum periods of heart rate> 120 bpm and frequency heart rate <50 bpm, supraventricular ectopy (SVE), ventricular ectopy (VE), pauses (> 2s), depression or ST segment elevation, autonomic modulation, reported symptoms during the test (and its association with arrhythmia).
Three classes of supraventricular ectopy (SVE) were studied: isolated ESV, non-sustained atrial tachycardia (<30s SVE) and sustained atrial tachycardia (>30s of symptomatic atrial tachycardia or SVE). The criteria should include identification of the three SVE: prematurity, a post-contraction and morphology. Assuming that only the excess of supraventricular arrhythmias could have clinical importance, classified as supraventricular electrical instability in the presence of high incidence> 30 SVE/h and/or> following 30 SVEs. Patients with <10 SVE/h were classified as low incidence of electrical instability and those with> 10 SVE/h <30 SVE/h as the average incidence of electrical instability. The ventricular ectopy were classified as isolated or complex (polymorphic, in bigeminy, paired).
The presence of> 30 VE/h were classified as ventricular electrical instability of high incidence. The presence of> 10 VE/h <30 VE/h as ventricular electrical instability and when the average incidence was <10 VE/h classified as ventricular electrical instability of low incidence. Were considered clinically significant when pauses lasting> 2s. The ST segment in the three channels was investigated for possible elevations or depressions. The reported symptoms and their association with arrhythmias have been described. Assessment of autonomic modulation was performed with analysis of the frequency and time domains of RR variability and classified as preserved or reduced autonomic modulation. In all visits were performed conventional electrocardiograms. The Ethics and Research of the National Heart Institute approved this study in 02/02/10 under number 0257.
The surgeries were performed through conventional median sternotomy, with cardiopulmonary bypass and mild hypothermia. For myocardial protection cold blood cardioplegia was infused in antegrade or retrograde via intermittently. Access to the mitral valve was performed through the left atrium in most cases.
The ablation lines were defined as:
1) Isolation of the pulmonary veins: the pulmonary vein isolation was achieved wrapping the right and left pulmonary veins in pairs, in an epicardial manner (passing one of the electrodes of the ablation device later and the other prior to the pulmonary veins), during cardiac decompression with cardiopulmonary bypass and therefore the patient heparinized, with the convexity of the device facing the left atrium to save the ostia of the pulmonary veins, and before the primary cardiac procedure, applying at least three periods of energy until the buzzer of the occurrence of transmural lesion at the same point.
2) left atrial connecting lines: lines of connection between the pair of right and left pulmonary veins were performed after opening the left atrium by placing one electrode on the outside of the LA posterior wall (epicardium) and the other inside (endocardium), such that the ablation lines performed previously for the isolation of the pulmonary veins were connected upper and/or inferiorly. This procedure was performed during the primary cardiac procedure.
3) Line of connection to the mitral annulus: the connecting line to the mitral annulus was not performed with the bipolar radiofrequency clamp for anatomical impossibility. This, when performed, was done using the technique of cut and suture, connecting the mitral valve annulus to the line of isolation of right inferior pulmonary vein.
4) Cavotricuspid line: cavotricuspid line was performed using the RFB clamp encompassing the right atrial free wall after its opening, in such a way to communicate the atriotomy line to the tricuspid ring, after the coronary sinus ostium venosus.
5) Cava-cava line: with the patient under cardiopulmonary bypass and aorta clamped, through small hole in the right atrial free wall, one ablation clamp leg was introduced toward the superior vena cava and then the inferior vena cava, so that the atrial tissue stays enclosed by two clamp legs during delivery of bipolar energy. When the right atrium was opened for access to the tricuspid valve, the same lesions were performed from the atrial incision.
Characteristics of patients
Of the 53 patients, 34 (64%) were women and ages ranged from 27 to 72 years (mean: 49.3 years ± 10.7 years). The mean duration reported of AF was 41 months (range 3-192 months). The type of AF was presented: eight patients in paroxysmal AF, persistent in three and permanent in 42. The left atrium had an average size of 52.9 ± 8.5 mm, ranging from 48 to 79 mm and the mean ejection fraction (LVEF) was 59% ± 13%. One patient had prior pacemaker and none had been submitted prior to the ablation of any arrhythmia. Four patients had a history of previous cerebrovascular accident (CVA). The events related to AF were observed in four patients. One patient showed complete resolution of neurological symptoms at the time of surgery and three remained with mild language and motor sequelae.
The types of injuries that led to mitral surgery were mitral stenosis in 32 patients, mitral regurgitation in 15 and mitral lesion in six. One patient had active infective endocarditis of the mitral valve causing regurgitation. In total, 10 surgeons were responsible for the surgery.
RESULTS
There were seven (13%) intraoperative deaths and survival after 14 months was 87%. The causes of perioperative deaths were five deaths from cardiogenic shock (two cases of atrioventricular disjunction) and two deaths from septic shock. The two cases of atrioventricular disjunction were diagnosed still during surgery and in both it was tempted surgical suture of the atrioventricular junction with bovine pericardium, but without success. This surgical accident was not associated with surgical ablation, since the lines of injury in both cases were performed away from the mitral annulus.
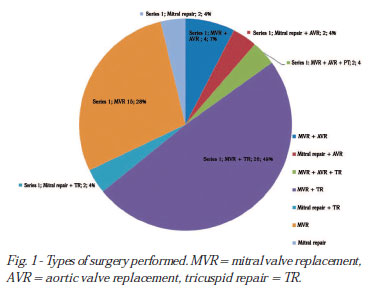
The surgeries performed were: 47 mitral valve replacement (27 biological and 14 metal) and six mitral valve repair. In 30 patients, it was associated tricuspid valvuloplasty in eight aortic valve replacement (seven metal and one organic), and three of them, closure of patent foramen ovale (Figure 1).
Of the 46 surviving patients, eight (17.3%) did not perform 24 hour Holter or ECG after 6 months after surgery, period which the presence of supraventricular tachycardia is considered therapeutic failure. The reason for this failure was: one moved from state and the another could not be contacted by telephone and six gave up the exam or attend the consultation. Of the 38 patients with ECG findings after 6 months of surgery, all had conventional electrocardiogram and 34 underwent 24 hour Holter (performed at a mean of 430 ± 123 days after surgery, ranging from 176 to 763 days).
24 hour Holter and conventional ECG revealed the following rhythms: sinus in 25 (66%) patients, AF in seven (18%), Flutter in five (13%) and junctional in one (3%). Therefore, 26 of 38 (68%) patients were free of tachyarrhythmias after 14 months postoperatively. 24h Holter information can be seen in Table 1.

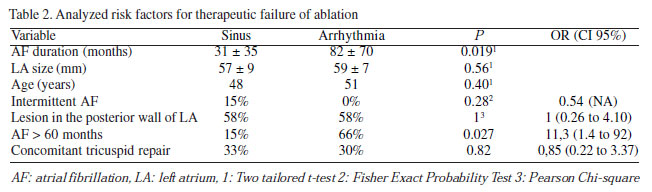
We studied potential risk factors for therapeutic failure: AF duration prior to surgery, left atrial size, age, type of AF and achievement or not of lesions in the posterior wall of left atrium. The only risk factor who showed clinically and statistically significant was the greatest time of AF preoperatively, as shown in Table 2. Patients with AF for more than 60 months had an OR of 11.3 for therapeutic failure.
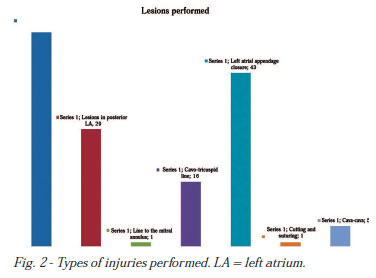
The set of ablation lines performed can be assessed in Figure 2. The need to implant a permanent pacemaker postoperatively was zero.
Regarding the use of antiarrhythmic medication, among 37 patients with ECG findings after 6 months of surgery, 11 were not using any drugs, 8 were in use of amiodarone only, 10 in use of atenolol only, four in use of amiodarone and atenolol and seven are missing information. Regarding the use of anticoagulants and/or antiplatelet, two were not using any of these, 30 were taking warfarin, one using ASA and five no information. Of the 26 patients in sinus rhythm, seven used no antiarrhythmic and five did not use coumarin.
One patient had neurological events in the postoperative period, with complete resolution of symptoms after 7 days.
Percutaneous ablation of residual or recurrent arrhythmias was performed in only one patient for treatment of right atrial flutter successfully, 9 months after surgery.
DISCUSSION
The bipolar radiofrequency is one of many alternative forms of energy used to attempt to reproduce the lesions made by cutting and suture during the Maze III procedure for the surgical treatment of atrial fibrillation. In our country, its feasibility, safety and efficacy have been demonstrated recently by Canale et al. [6] in a heterogeneous group of patients undergoing cardiac surgery, in general, with maintenance of sinus rhythm after 1 year of 76%. Other forms of energy were studied by the authors in our country, such as unipolar radiofrequency by Breda et al. [7] and Abreu Filho et al. [8], showing mixed results and the use of ultrasound by Brick et al. [9]. However, as far as best of our knowledge, this is the first national experience of exclusive study of patients with rheumatic mitral valve disease using a bipolar radiofrequency.
Most studies of surgical treatment of atrial fibrillation comprises patients with degenerative mitral regurgitation. It is known that this group of patients is different from those with rheumatic mitral valve disease. Rheumatic disease affects not only the heart valves, but also causes chronic inflammation in the atria, leading to fibrosis and muscle fibers [10]. Electrical remodeling of the left atrium has been described in these patients, leading to higher propensity to develop atrial fibrillation [11]. The most common complication of mitral stenosis is rheumatic AF and its prevalence increases as the severity of valve obstruction and the patient's age. Therefore, the presence of AF in patients undergoing mitral valve surgery for rheumatic origin is extremely common, but specific treatment in this subgroup is less studied.
The comparison between AF patients with degenerative and rheumatic disease, keeping all other risk factors for controlled therapeutic failure (size of LA, AF duration, age), is very difficult by the large number of patients required for this. Therefore, in the scientific literature, are predominant the reports on safety and efficacy in the treatment of concomitant AF in patients undergoing mitral valve surgery for rheumatic etiology. Guang et al. [12] compared 96 patients with rheumatic mitral valve disease who also underwent AF ablation, with only 87 patients undergoing mitral valve surgery. The maintenance of sinus rhythm after 3 years was significantly higher in the group undergoing ablation (77%) compared to those without ablation (25%). Cui et al. [13] reported 74.5% of sinus rhythm after 12 months of surgery in a group of 91 patients comprising mostly rheumatic, with persistent/permanent AF, using RFB.
In this study, three different sets of lesions were used (Cox-Maze III, Cox Mini-Maze and modified left Maze), with no difference between them as to the outcome of sinus rhythm. Abreu Filho et al. [14] performed interesting randomized study in patients with isolated rheumatic mitral valve disease and permanent atrial fibrillation using unipolar ablation device (SICTRA). Seventy patients were assigned randomly to be submitted only to mitral valve surgery or mitral valve surgery concomitant with unipolar ablation of modified Maze III type. The study revealed not only the efficacy of ablation in this group of patients with rheumatic disease only (79.4% of sinus rhythm after 1 year follow-up) but also to demonstrate the low efficacy of treating only the mitral valve with respect to heart rate: 26 9% of sinus rhythm only. In this study, there were no accidents related to ablation.
In our series, the therapeutic failure of 31% is comparable to reports in the literature. However, we believe there is possibility for improvement in the future regarding the execution of the most complete lines of ablation, especially those of the posterior wall of the LA. Only 29/53 (54%) patients received posterior communication line of LF, while 45/53 (85%) had persistent or permanent AF, a group that theoretically should receive this injury.
Some studies involving patients with different etiologies for mitral valve disease who underwent AF ablation concomitantly recognize rheumatic ethiology as a risk factor for failure of ablation therapy in univariate analysis. Fayad et al. [15], assessing 70 patients who underwent left atrial ablation only, exclusively in individuals with mitral valve disease, identified rheumatic ethiology as a risk factor for AF return. After 2 years of follow-up, 62.5% of patients were in sinus rhythm. On the other hand, Chen et al. [16] when assessing 99 patients with persistent AF undergoing mitral valve surgery for various reasons associating them to the RFB ablation, found the rheumatic etiology as a risk factor for postoperative AF. In this study, only LA size and AF duration were determinants of the rhythm in the 2-years follow-up.
Some randomized studies of AF ablation using various alternative energy sources show that the benefits are found in the dimensions of symptoms and decreased use of medications. von Oppell et al. [17] randomized 50 patients for mitral valve surgery with or without concomitant AF ablation. Those who remained in sinus rhythm had better scores on quality of life questionnaires and were more in free use of anticoagulants and antiarrhythmics. However, mortality and thromboembolic events during follow-up were low and similar in both groups. Doukas et al. [18] in a randomized study of 97 patients found low efficacy of ablation (45% in one year), but it was possible to determine the benefits of maintaining sinus rhythm, especially the main and most functional capacity in walk test and smaller serum B-type natriuretic peptide. It was not possible to find differences in mortality or embolic complications during one year of follow-up.
Among the classics and more recognized risk factors for treatment failure in AF ablation (age, left atrial size and AF duration), we found as significant only the time of AF before surgery. However, this proved to be highly predictive of failure of ablation. Patients with AF history of more than 5 years are 11.3 times more likely to continue at a AF/flutter rhythm than patients with less than 5 years. In our sample, it becomes a good predictor of treatment failure and serve as a marker to exclude patients for ablation by the high failure rate. Similarly, Chen et al. [16] found an OR of 9.45 for therapeutic failure in patients with AF duration prior to surgery more than 66 months.
The mortality rate in our sample (13%) reflects the severity of the disease and the late moment in which these patients are referred for surgery. The presence of AF in itself demonstrates mitral valve disease evolved. Another characteristic of our sample is the high frequency of multivalvular patients. Only 17/53 (32%) were patients with isolated mitral valve disease. Twenty-eight (53%) patients underwent, in addition to mitral valve surgery, concomitant tricuspid valve repair. Six (11%) patients needed mitral-aortic and two (4%) trivalvular surgery (double mitral-aortic and tricuspid valve replacement).
The 24-hour Holter is an important tool to assess recurrence of AF/flutter after any ablative procedure [19]. However, in addition to generating information about heart rate and thus detect failures of ablation, it may also investigate the association between symptoms and heart rate, presence of supraventricular and ventricular ectopy, preservation of autonomic modulation and help heart rate control. In reviewing all the 24 hour Holter tests performed in this sample, some data gain importance. The presence of excessive supraventricular ectopia (> 30SVE/h) in patients in sinus rhythm was common (5/24, 21%) as well as the incidence of non-sustained atrial tachycardia (41%). The importance of the excessive presence of supraventricular ectopia as a risk factor for atrial fibrillation, stroke and death was well established in a large healthy population sample studied by 48-hour Holter [20]. In this study, the high incidence of supraventricular activity (we use the same definition) was found in 14.6% of subjects and was associated in the monitoring of more than six years, with a greater chance of the composite outcome of death/stroke (HR: 1.64) and hospital admission for HF (HR: 2.78). Engström et al. [21] also outlined strong correlation between men with excessive supraventricular activity (> 218 SVE/24h) and increased risk of stroke (RR: 1.9).
Our sample has a higher prevalence of individuals with high incidence of supraventricular activity (21%), but the importance of this condition in the context of late postoperative ablation has not yet been investigated. In our environment, Cunha et al. [22] quantified the incidence of supraventricular ectopia in the late postoperative period of Cox-Maze III associated to valvular surgery, finding an average of 2.3% of heart rate as derived from atrial ectopy and 35% presenting non-sustained atrial tachycardia.
The importance of 24 hour Holter in our context can be also included in the adjustment of medications that control the heart rate. Twelve percent of patients had prolonged pauses (> 2s) and 24% had some time with HR <60 bpm, all associated with high doses of amiodarone and/or beta blockers.
The reduced autonomic modulation was found in 46% of those in which it could be assessed (it is not possible to assess in patients with sustained tachyarrhythmia). This finding may be explained by a process of sympathetic and parasympathetic denervation resulting from multiple mechanical injuries made in the atria.
Nine (26%) patients reported symptoms during the test, but in only two of them (22%) the symptom was associated with rhythm disorder, showing how weak is the correlation between symptoms and arrhythmias in this context. Cunha et al. [22] reported a similar experiment, revealing that 41% of patients in their sample reported symptoms during the examination, but only 43% of them exhibited electrical substrate at the time of the symptom.
Limitations of the study
This study has several limitations. It is retrospective and open. The number of patients studied is small, which can compromise the analysis of risk factors for therapeutic failure. Some traditional risk factors such as size of LA and type of AF, were not significant in this series. In addition, our loss of monitoring is high (17%). All surgeons involved in the surgeries were in the process of learning curve with this method.
CONCLUSIONS
The use of bipolar radiofrequency for the treatment of atrial fibrillation in patients undergoing surgery for rheumatic mitral valve is effective in controlling the arrhythmia in 68% of patients after 14 months. The duration of preoperative AF was an important predictor of treatment failure. The 24 hour Holter, in addition to detect arrhythmias, adds relevant information such as supraventricular ectopic excessive activity, assessment of autonomic modulation and correlation between symptoms and electrocardiographic events.
REFERENCES
1. Benjamin EJ, Wolf PA, D'Agostino RB, Silbershatz H, Kannel WB, Levy D. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998;98(10):946-52. [MedLine]
2. Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991;22(8):983-8. [MedLine]
3. Geidel S, Ostermeyer J, Lass M, Boczor S, Kuck KH. Surgical treatment of permanent atrial fibrillation during cardiac surgery using monopolar and bipolar radiofrequency ablation. Indian Pacing Electrophysiol J. 2003;3(3):93-100. [MedLine]
4. Albrecht A, Kalil RA, Schuch L, Abrahão R, Sant'Anna JR, Lima G, et al. Randomized study of surgical isolation of the pulmonary veins for correction of permanent atrial fibrillation associated with mitral valve disease. J Thorac Cardiovasc Surg. 2009;138(2):454-9. [MedLine]
5. Shemin RJ, Cox JL, Gillinov AM, Blackstone EH, Bridges CR; Workforce on Evidence-Based Surgery of the Society of Thoracic Surgeons. Guidelines for reporting data and outcomes for the surgical treatment of atrial fibrillation. Ann Thorac Surg. 2007;83(3):1225-30. [MedLine]
6. Canale LS, Colafranceschi AS, Monteiro AJ, Coimbra M, Weksler C, Koehler E, et al. Uso da radiofrequência bipolar para o tratamento da fibrilação atrial durante cirurgia cardíaca. Arq Bras Cardiol. 2011;96(6):457-64.
7. Breda JR, Breda ASCR, Meneguini A, Freitas ACO, Pires AC. Ablação operatória da fibrilação atrial por radiofrequência. Rev Bras Cir Cardiovasc. 2008;23(1):118-22. [MedLine]
8. Abreu Filho CAC, Dallan LAO, Lisboa LAF, Spina GS, Scanavacca M, Grinberg M, et al. Resultados da ablação cirúrgica por radiofrequência da fibrilação atrial crônica. Rev Bras Cir Cardiovasc. 2004;19(3):301-8.
9. Brick AV, Seixas TN, Portilho CF, Peres AK, Vieira Jr JJ, Melo Neto R, et al. Tratamento intra-operatório da fibrilação atrial crônica com ultra-som. Rev Bras Cir Cardiovasc. 2001;16(4):337-49. View article
10. Otto CM, Bonow RO. Valvular heart disease. In: Libby P, Bonow RO, Mann DL, Zipes DP, eds. Braunwald's heart disease: a textbook of cardiovascular medicine. Philadelphia:Elsevier;2008. p.1649.
11. John B, Stiles MK, Kuklik P, Chandy ST, Young GD, Mackenzie L, et al. Electrical remodelling of the left and right atria due to rheumatic mitral stenosis. Eur Heart J. 2008;29(18):2234-43. [MedLine]
12. Guang Y, Zhen-jie C, Yong LW, Tong L, Ying L. Evaluation of clinical treatment of atrial fibrillation associated with rheumatic mitral valve disease by radiofrequency ablation. Eur J Cardiothorac Surg. 2002;21(2):249-54. [MedLine]
13. Cui YQ, Meng X, Li Y, Wang JG, Zeng W, Gao F, et al. Intraoperative treatment for atrial fibrillation using bi-polar radiofrequency ablation system: a clinical report of 91 cases. Zhonghua Wai Ke Za Zhi. 2009;47(7):533-6. [MedLine]
14. Abreu Filho CA, Lisboa LA, Dallan LA, Spina GS, Grinberg M, Scanavacca M, et al. Effectiveness of the maze procedure using cooled-tip radiofrequency ablation in patients with permanent atrial fibrillation and rheumatic mitral valve disease. Circulation. 2005;112(9 Suppl):I20-5. [MedLine]
15. Fayad G, Le Tourneau T, Modine T, Azzaoui R, Ennezat PV, Decoene C, et al. Endocardial radiofrequency ablation during mitral valve surgery: effect on cardiac rhythm, atrial size, and function. Ann Thorac Surg. 2005;79(5):1505-11. [MedLine]
16. Chen MC, Chang JP, Chang HW, Chen CJ, Yang CH, Chen YH, et al. Clinical determinants of sinus conversion by radiofrequency maze procedure for persistent atrial fibrillation in patients undergoing concomitant mitral valvular surgery. Am J Cardiol. 2005;96(11):1553-7. [MedLine]
17. von Oppell UO, Masani N, O'Callaghan P, Wheeler R, Dimitrakakis G, Schiffelers S. Mitral valve surgery plus concomitant atrial fibrillation ablation is superior to mitral valve surgery alone with an intensive rhythm control strategy. Eur J Cardiothorac Surg. 2009;35(4):641-50. [MedLine]
18. Doukas G, Samani NJ, Alexiou C, Oc M, Chin DT, Stafford PG, et al. Left atrial radiofrequency ablation during mitral valve surgery for continuous atrial fibrillation: a randomized controlled trial. JAMA. 2005;294(18):2323-9. [MedLine]
19. Calkins H, Brugada J, Packer DL, Cappato R, Chen SA, Crijns HJ, et al. Heart Rhythm Society; European Heart Rhythm Association; European Cardiac Arrhythmia Society; American College of Cardiology; American Heart Association; Society of Thoracic Surgeons. HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for personnel, policy, procedures and follow-up. A report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation developed in partnership with the European Heart Rhythm Association (EHRA) and the European Cardiac Arrhythmia Society (ECAS); in collaboration with the American College of Cardiology (ACC), American Heart Association (AHA), and the Society of Thoracic Surgeons (STS). Endorsed and approved by the governing bodies of the American College of Cardiology, the American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons, and the Heart Rhythm Society. Europace. 2007;9(6):335-79. [MedLine]
20. Binici Z, Intzilakis T, Nielsen OW, Køber L, Sajadieh A. Excessive supraventricular ectopic activity and increased of atrial fibrillation and stroke. Circulation. 2010;121(17):1904-11. [MedLine]
21. Engström G, Hedblad B, Juul-Möller S, Tydén P, Janzon L. Cardiac arrhythmias and stroke: increased risk in men with high frequency of atrial ectopic beats. Stroke. 2000;31(12):2925-9. [MedLine]
22. Cunha B, Kalil RA, Albrecht AS, Lima GG, Kruse JC. Evaluation of the heart rate and arrhythmias following the maze procedure for chronic atrial fibrillation. Arq Bras Cardiol. 1999;72(5):607-14. [MedLine]
Article receive on Sunday, August 7, 2011
 All scientific articles published at rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at rbccv.org.br are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()
 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}