![]()
![]()
Debora Cristina Fontes LeiteI; José Teles de MendonçaII; Rosana CipolottiIII; Enaldo Viera de MeloIV
DOI: 10.5935/1678-9741.20120038
ABSTRACT
OBJECTIVE: This study aims evaluate the treatment of congenital heart disease conducted from 2000 to 2009.
METHODS: The sample consisted of all patients undergoing surgical correction for congenital heart disease for ten years in Sergipe, Brazil. The patients were operated in three hospitals located in the city of Aracaju, capital of the state of Sergipe (Brazil). The study was divided into two periods defined by the start date of centralization of surgery. The variables collected were: age, sex, postoperative diagnosis, destination, type of surgery and hospital where the procedure was performed and the classification RACHS -1.
RESULTS: In the period I, the estimate deficit of surgery was 69% decrease occurring in the period II to 55.3%. The postoperative diagnosis was more frequent closure of the interventricular communication (20.5%), closure of patent ductus arteriosus (20.2%) and atrial septal defect (19%). There was a statistically significant correlation between the expected mortality RACHS-1 and observed in the sample. The evaluation of RACHS-1 as a predictor of hospital mortality by ROC curve showed area of 0.860 95% CI 0.818 to 0.902 with P <0.0001.
CONCLUSION: The results of this study indicate that the centralization and organization of existing resources are needed to improve the performance of surgical correction of congenital heart diseases.
RESUMO
OBJETIVO: Avaliar o tratamento das cardiopatias congênitas realizadas de 2000 a 2009.
MÉTODOS: A amostra constituiu-se de todos os pacientes submetidos a correção cirúrgica para cardiopatias congênitas por dez anos em Sergipe, Brasil. Os pacientes foram operados em três hospitais localizados na cidade de Aracaju (SE, Brasil), capital do estado de Sergipe. O estudo foi dividido em dois períodos, definidos pela data do início da centralização das cirurgias. As variáveis coletadas foram: faixa etária, gênero, diagnóstico pós-operatório, destino, tipo de cirurgia e hospital em que foi realizado o procedimento e a classificação RACHS -1.
RESULTADOS: No período I, a estimativa do déficit de cirurgia foi de 69%, ocorrendo decréscimo no período II para 55,3%. O diagnóstico pós-operatório mais frequente foi de fechamento de comunicação interventricular (20,5%), fechamento de canal arterial (20,2%) e da comunicação interatrial (19%). Houve correlação estatisticamente significativa entre mortalidade esperada pelo RACHS-1 e a observada na amostra. A avaliação do RACHS-1 como fator preditor da mortalidade hospitalar por meio da curva ROC demonstrou área de 0,860 IC 95% 0,818 a 0,902, com P < 0,0001.
CONCLUSÃO: Os resultados deste estudo indicam que a centralização e a organização dos recursos existentes são necessárias para melhora no desempenho das correções cirúrgicas das cardiopatias congênitas.
CPB: cardiopulmonary bypass
IAC: interatrial communication
IVC: interventricular communication
AC: Aortic coarctation
AVSD: Atrioventricular Septal Defect
CI: Confidence Interval
PDA: Patent ductus arteriosus
RACHS-1: Risk Adjustment for Congenital Heart Surgery
ROC: Receiver-Operating Characteristic curve
SUS: Unified Health System
RV: Right ventricle
LV: Left ventricle
INTRODUCTION
The many advances made in cardiac surgery in the world last year [1] are often not accessible to people in developing countries [2].
Recently, in several developing countries, strategies were proposed for correction of congenital heart diseases, such as transfer of patients to developed countries, arrangement of cardiac surgeons' trips to these countries or the creation of a local cardiovascular surgery program [3-6].
Brazil has several developments within cardiac surgery [7], but when comparing to other countries, shows a deficit of surgery for correction of congenital heart disease estimated at around 65%, depending on the region, with the northern region (93.5%) and Northeast (77.4%) with the major deficits [8-10].
In Sergipe, since 2007, through an agreement with the Health System all surgical correction of congenital heart disease are performed in an institution, which previously was distributed in three services. The aim of this study is to assess the treatment of congenital heart disease performed from 2000 to 2009, comparing the periods before and after the surgeries centralization.
METHODS
Sampling was performed consecutively, collected retrospectively, and all patients underwent surgical correction for congenital heart disease from January 1st, 2000 to December 31th, 2009 in Sergipe.
The patients underwent surgery in three hospitals located in the city of Aracaju, capital of Sergipe State, being designated hospital 1, 2 and 3, for ethical reasons. Data from these patients were collected from the records of cardiopulmonary bypass (CPB), of compulsory filling, stored in single file, pertaining to all departments of cardiovascular surgery of Sergipe. The study was divided into two periods defined by the starting date of the agreement between SUS (Unified Health System-UHS) and the hospital 3, the period called I runs from January 1st, 2000 to December 31, 2006 and the period II from January 1st, 2007 to December 31th, 2009. The hospital is a charity institution that serves mostly UHS patients. The hospital 2, private, serves mostly patients from health plans and private, having an agreement with the UHS to perform heart surgery. Due to difficulties encountered in these hospitals for surgeries in pediatric patients, an agreement between UHS and the Hospital 3 was signed centralizing all procedures in the pediatric population in this service.
The data collection of surgical correction was performed from July to December 2010. The variables collected were: age, gender, postoperative diagnosis, destination (discharge or death), type of surgery and hospital where the procedure was performed.
The age range was established in the neonatal period (1-28 days old), 1st year of life (29 days to <1 year), children (from 1 year to 12 years) and adolescents and adults (over 12 years). We adopted the definition of the Brazilian Statute for Children and Adolescents establishing pediatric patients up to 12 years. For analysis of hospital mortality, child age was grouped with the adult, for statistical reasons, because there were no deaths in the latter.
In the CPB record there was description of the pre-and postoperative diagnosis being considered in this study only the latter. From the postoperative diagnosis and the type of surgery were categorized in the classification of surgical risk for congenital heart disease according Risk Adjustment for Congenital Heart Surgery (RACHS-1) [11].
For death, we considered those occurring during the hospitalization and so-called hospital mortality.
Were requested from the Health Secretary of Sergipe official birth certificate from 2000 to 2009.
Due to difficulties in the diagnosis of congenital heart disease, we chose to assess the deficit of corrective surgery of congenital heart disease through estimates of disease incidence in relation to the number of live births, according to the methodology used in the literature [12].
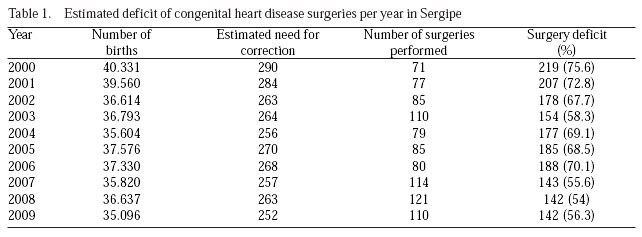
We calculated the estimated deficit of surgery, where from the prevalence of the disease, 8 in 1000 live births, and the need for surgery in 80% of cases (7.2 per 1000 live births), we calculated the number of surgeries performed each year and subtracting the number of surgeries performed, it was the annual deficit.
Categorical variables were described as single frequency (count) and percentages and their 95% CI (confidence interval for an estimated 95%) when appropriate.
To assess the association between categorical variables we used the chi-square test. The analysis of expected mortality and by RACHS -1 and that observed in the sample were performed by Pearson correlation. For assessment of hospital mortality and RACHS-1 was constructed ROC curves and estimated the area under it.
We considered the significance level as P <0.05, power 0.80 and the tests as two-tailed.
The statistical software used was SPSS version 17 for testing.
This study was submitted to the Ethics in Research Involving Human Committee at the Federal University of Sergipe and approved in May 2010.
RESULTS
There was a deficit reduction of surgeries of 75.6% in 2000 to 54% in 2008, the year with lowest deficit. There was significant reduction of the surgery deficit over the years with P <0.0001. In relation to the periods of study, in the period I the estimated deficit of surgery was 69%, with decrease in period II to 55.3% (Table 1).
In terms of age we observed a higher frequency of surgery in the age group 1-12 years, followed by over 12 years, with the smallest percentage in the neonatal period. Comparing the periods of the study, 15.5% of patients younger than one year underwent surgery in the period I and 20.3% in period II (Table 2).
According to the postoperative diagnosis, the most frequent correction was closure of interventricular communication (IVC) (20.5%), closure of the ductus arteriosus (20.2%) and interatrial communication (IAC) (19%) (Table 3).

In the classification of surgical risk for congenital heart defects by RACHS-1 there it was more common in categories 1 and 2, not occurring in category 5 in the ten years of follow-up (Table 4).

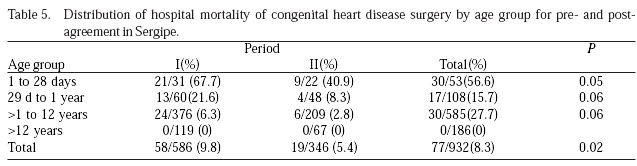
Of the 932 patients undergone surgery, 77 (8.3% CI 95% 6.5 to 10.1) have evolved to death during hospitalization, and the neonatal age group had the highest rate of death (56.6%) and death not occurring in patients over 12 years (Table 5).
Regarding the RACHS-1 risk classification the higher frequency of hospital mortality occurred in higher risk categories (4/6), however, with statistically significant difference between the periods, with reduced mortality in the period II, P <0, 0001 (Fig. 1).

There was a statistically significant correlation (adjusted R2 = 0.977 and P< 0.0001) between expected mortality by RACHS-1 and observed in the sample.
The assessment of the RACHS-1 as a predictor of hospital mortality by ROC curve showed area of 0.860 95% CI 0.818 to 0.902 with P <0.0001 and statistically significant and comparable to that found in the literature [9] (Fig. 2].

DISCUSSION
In the present study data, the number of surgeries over the years shows the increasing trend year by year from 2000 to 2003. Between 2004 to 2006 there was a decrease with increasing number of surgeries after 2007. This represents, numerically, the crisis experienced by the pediatric cardiac surgery between 2004 and 2006 which led to the centralization of infrastructure and human resources in the hospital 3, making productivity returned in 2003, Table 1.
There was reduction in surgery deficit to 56% in period II, a value close to the estimated deficit in the Southeast region, site of the largest number of surgeries and centers for cardiovascular care [10].
Most surgeries occurred between age 1-12 years in two periods, being always the neonatal age group with the lowest ratio, followed by the age of 29 days to one year, according Table 2. This data serves as another indicator of deficit, because half of the repairs should have been performed up to the 1st year of life [13]. With the centralization of activities in the hospital 3, this increased proportion of children who underwent surgery before 1 year of 15.5% to 20.3% after the agreement, however, not statistically significant, probably due to sample size (Table 2).
As described in the literature, 20% of patients undergoing repair of congenital heart disease were in the adult age group (table 2), a fact that did not change between periods (Table 4). This finding reinforces the deficit of surgical correction, since no patient had to postpone the procedure to adulthood, when some changes are already irreversible [12].
In period II a partnership with the Service of Mobile Emergency Care was organized, responsible for transport between units and hospitals for the early return of newborns to neonatal intensive care, generating turnover of intensive care beds and, consequently, increasing the number of surgeries.
With respect to postoperative diagnosis, the frequency of correction of the interventricular septum defect was 20%, slightly below the described in the literature [14]. However, the frequency of IAC (19%) and PDA (20%) were well above those described in the literature [15,16]. Probably the surgeries deficit associated with the fact these more benign pathologies bear the delay in repair caused the cumulative frequency of these pathologies.
Tetralogy of Fallot, with 12.3% of cases, was similar to the frequency found in the literature [17], also the Total Atrioventricular Septal Defect with 3.3% and Pulmonary Atresia with 3.6% of cases [18]. The aortic coarctation, with frequency in the literature of 5-8%, appears lower than expected with 2.1% of cases [19].
The pulmonary stenosis with 4.1% and transposition with 2.3% of cases were below the reported in the literature [18]. However, as the study approached surgical repairs and it is very serious diseases, probably the difference is the number of patients who progressed to death before surgical opportunity.
The agreement with UHS reflected the reduction in hospital mortality of 9.8% in the pre-agreement to 5.4% in the post-agreement (Table 5), mainly with a reduction in the neonatal period, where there was statistical significance and in the other age groups there was no statistical significance probably due to the number of cases, but the total number of surgeries we realize the impact of the reduction with P <0.02.
The association between higher volume of cases and better patient outcomes has been demonstrated for several surgical procedures and medical treatments, including surgery for children with congenital heart disease. In this context, centers with fewer than 70 procedures per year are considered low productivity, between 70 to 110 of productivity average and more than 110 procedures are considered as high productivity. The centers with higher productivity present better results [20,21].
The agreement between UHS and Hospital 3, which divides the study periods, promoted the centralization of the flow of patients with congenital heart disease in the pediatric population for this institution. The number of surgeries performed in the period I was of low productivity, because it was divided between the Hospital 1, which received more complex patients, and Hospital 2, which admitted patients with better prognosis. In period II, the surgeries of patients under 12 years were performed at Hospital 3, and the number of procedures already ranks as of average productivity.
With increase in the number of surgeries per year the support team becomes well prepared, which for major surgery and the need for adequate infrastructure is of great importance, impacting the outcomes. Grouped by RACHS-1 risk classification between the periods, it is clear the reduction in mortality, especially among the categories 2, 3 and 4, lower risk class, Table 5.
Therefore, the centralization of material and human resources had as benefit the increasing number of surgeries, as well as the surgical outcomes with reduced hospital mortality rates, even when assessing the severity of cases.
In linear regression between the RACHS-1 risk classification and hospital mortality it is clearly demonstrated that there are statistically significant correlation and that is a valid instrument for use in our country [9].
CONCLUSION
The outcomes of this study indicate that the centralization of both human resources and infrastructure are important for surgery of congenital heart disease, and the organization of existing resources is necessary to improve the performance of the service.
ACKNOWLEDGMENTS
We thank all congenital heart surgery team, the pediatric cardiologists, postoperative intensivists in Sergipe in the determination and tenacity facing clinical and socio-economics challenges of our time.
REFERENCES
1. Lisboa LAF, Moreira LFP, Meija OV, Dallan LAO, Pomerantzeff PMA, Costa R, et al. Evolução da cirurgia cardiovascular no Instituto do Coração: análise de 71.305 operações. Arq Bras Cardiol. 2010;94(2):174-81.
2. Yacoub MH. Establishing pediatric cardiovascular services in the developing world: a wake-up call. Circulation. 2007;116(17):1876-8. [MedLine]
3. Larrazabal LA, Jenkins KJ, Gauvreau K, Vida VL, Benavidez OJ, Gaitán GA, et al. Improvement in congenital heart surgery in a developing country: the Guatemalan experience. Circulation. 2007;116(17):1882-7. [MedLine]
4. Arzola RC, Sosa ES, Morejón CG, Casado JA, Lazo FV, Benavides AS, et al. Um nuevo enfoque de tratamiento integral del niño com cardiopatia em Cuba. Bol Oficina Saint Panam. 1994;117(3):275-6.
5. Gonzalez CL, Salazar BL, Salazar, VC. Cardiopatias congénitas en el Hospital México. Rev Med Costa Rica Centro Am. 2000;57(551):47-57.
6. Neirotti RA. Cardiac surgery: complex individual and organizational factors and their interactions. Concepts and practices. Rev Bras Cir Cardiovasc. 2010;25(1):VI-VII. [MedLine]
7. Stolf NA. Congenital heart surgery in a developing country: a few men for a great challenge. Circulation. 2007;116(17):1874-5. [MedLine]
8. Ministério da Saúde. MS/SVS/DASIS. Sistema de Informações sobre Mortalidade (SIM). Disponível em: http://www.datasus.gov.br/catalogo/sim.htm. Acesso em 7/7/2010.
9. Ithuralde M, Neirotti R. Neonatal heart surgery: evaluation of risk factors. NeoReviews. 2011;12:252-9.
10. Pinto Jr VC. Avaliação da Política Nacional de Atenção Cardiovascular de Alta Complexidade com foco na cirurgia cardiovascular pediátrica [Dissertação de Mestrado]. Fortaleza: Universidade Federal do Ceará; 2010.
11. Jenkins KJ, Gauvreau K, Newburger JW, Spray TL, Moller JH, Iezzoni LI. Consensus-based method for risk adjustment for surgery for congenital heart disease. J Thorac Cardiovasc Surg. 2002;123(1):110-8. [MedLine]
12. Pinto Jr VC, Rodrigues LC, Muniz CR. Reflexões sobre a formulação de política de atenção cardiovascular pediátrica no Brasil. Rev Bras Cir Cardiovasc. 2009;24(1):73-80. [MedLine] View article
13. Atik E, Atik FA. Momento da indicação cirúrgica das cardiopatias congênitas cianogênicas. In Souza AGMR, Mansur AJ, eds. Socesp Cardiologia. 2º vol. São Paulo:Atheneu;1996. p.813-28.
14. Myague NI, Cardoso SM, Meyer F, Ultramari FT, Araújo FH, Rozkowisk I, et al. Epidemiological study of congenital heart defects in children and adolescents. Analysis of 4,538 cases. Arq Bras Cardiol. 2003;80(3):269-78. [MedLine]
15. Furlanetto BHS, Martins TC. Defeito do septo atrioventricular. In: Croti UA, Mattos SS, Pinto Jr VC, Aiello VD, eds. Cardiopatia e cirurgia cardiovascular pediátrica. São Paulo:Roca;2008.
16. Silva LPRG, Bembom MC, Silva MFAG. Persistência do canal arterial. In: Croti UA, Mattos SS, Pinto Jr VC, Aiello VD, eds. Cardiopatia e cirurgia cardiovascular pediátrica. São Paulo:Roca;2008.
17. Valente AS, Cirino CMF. Cardiopatia congênita no adulto. In: Croti UA, Mattos SS, Pinto Jr VC, Aiello VD, eds. Cardiopatia e cirurgia cardiovascular pediátrica. São Paulo:Roca;2008.
18. Mattos SS, Crotti UA, Pinto Jr VC, Aiello VD. Terminologia. In: Croti UA, Mattos SS, Pinto Jr VC, Aiello VD, eds. Cardiopatia e cirurgia cardiovascular pediátrica. São Paulo:Roca;2008.
19. Ebaid M, Afiune JY. Coarctação de aorta: do diagnóstico simples às complicações imprevisíveis. Arq Bras Cardiol. 1998;71(5):647-8. [MedLine]
20. Chang RK, Klitzner TS. Can regionalization decrease the number of deaths for children who undergo cardiac surgery? A theoretical analysis. Pediatrics. 2002;109(2):173-81. [MedLine]
21. Novick WM, Anic D, Ivancan V, Di Sessa TG. International pediatric cardiac assistance in Croatia: results of the 10 year program. Croat Med J. 2004;45(4):389-95. [MedLine]
22. American College of Cardiology Foundation (ACCF). American Heart Association Methodology Manual for ACFF/ AHA Guideline Writing Committees: Methodologies and policies from the ACCF/AHA task force on practice guidelines. 2009. Disponível em:
23. Burstein DS, Rossi AF, Jacobs JP, Checchia PA, Wernovsky G, Li JS, et al. Variation in models of care delivery for children undergoing congenital heart surgery in the United States. Worid J Pediatr Congenit Heart Surg. 2010;1(1):8-14.
24. Smith PC, Powell KR. Can regionalization decrease the number of deaths for children who undergo cardiac surgery? A theoretical analysis. Pediatrics. 2002;110(4):849-50.
25. Mee RBB. Global challenges in education and training for congenital heart surgery: The Second Aldo Castañeda Lecture (2009). The second scientific meeting of the World Society for Pediatric and Congenital Heart Surgery at the Fifth world Congress of pediatric cardiology and Cardiac Surgery, Cairns, Queensland, Australia. Jun 21-26, 2009.
Article receive on Friday, October 28, 2011
 All scientific articles published at rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at rbccv.org.br are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()
 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}