![]()
![]()
Ebuzer Aydin; Akin Arslan; Mehmet Ozkokeli
DOI: 10.5935/1678-9741.20140045
ACC: American College of Cardiology
AHA: American Heart Association
CABG: Coronary Artery Bypass Grafting
CPR: Cardiopulmonary Resusitation
DVA: Valve De Vega Annuloplasty
ECG: Electrocardiogram
ECHO: Echocardiography
EF: Ejection Fraction
ESC: European Society of Cardiology
ICU: Intensive Care Unit
LA: Left Atrium
NYHA: New York Heart Association
PAP: Pulmonary Artery Pressure
RF: Radiofrequency
STA: Superior Transseptal Approach
INTRODUCTION
Good exposure is mandatory for mitral valve surgery, when the original valve is calcified or a previously implanted mitral prosthesis is removed. Mitral visualization may be insufficient due to the small size of the left atrium and markedly hypertrophic right ventricle. Previous cardiac operations may complicate mitral valve exposure, as adhesions and loss of mobility in the surrounding tissues may be present. In such cases, the conventional left atria1 incision may not offer satisfactory visualization in the surgical site of the valve. Therefore, several alternative approaches have been proposed for satisfactory visualization of the mitral valve intraoperatively[1-5].
Berreklouw et al.[2] and Guiraudon et al.[3] proposed a combined superior-transseptal approach to create a larger operation area which was closer to the mitral valve. Currently, this approach has been adopted by several health care centers[1]. On the other hand, there are possible drawbacks including increased ischemia time, cardiopulmonary bypass (CPB), cross-clamp time, and increased bleeding related to the procedure based on the current clinical experiences[4,5].
Cardiac arrhythmia is one of the main concerns with this procedure. Early atrial tachycardia has been frequently reported[6], while many studies have demonstrated that superior transseptal approach (STA) is commonly associated with sinus node dysfunction[4,7-10].
In this study, we aimed to compare clinical outcomes of STA with the conventional left atriotomy (LA) in patients undergoing mitral valve surgery.
METHOD
Patient selection
Between January 2010 and November 2012, a total of 91 consecutive adult patients who underwent mitral valve surgery in the Division of Cardiovascular Surgery at Koşuyolu Training and Research Hospital were included. The patients were randomized at a 1:1 ratio to either STA (Group 1, n=47) and conventional LA (Group 2, n=44). Pacemaker implantation criteria were predefined according to the American College of Cardiology / American Heart Association/the European Society of Cardiology (ACC/AHA/ESC) guidelines[11]. The study protocol was approved by the local Ethics Committee of our institution.
Surgery
Superior transseptal approach
A superior venous cannula was inserted directly from the superior vena cava, while an inferior venous cannula was inserted from inferior vena cava. Caval cannulas were inserted more laterally to the right atrium to avoid the appendage of right atrium. The right atriotomy was performed in parallel to the atrioventricular groove and the incision was carried superiorly to the appendage to meet the superior pole of the interatrial septum, leaving a strip of atrial tissue on the ventricular side to facilitate closure. The retrograde coronary sinus cannulation was performed under vision for the cardioplegia infusion. The aorta was cross-clamped and the heart was arrested with cold blood cardioplegia. The fossa ovalis was incised vertically and the septal incision was carried superiorly to meet the right atriotomy and extended for 2 to 3 cm to the roof of the left atrium. The ventricular side of the septal incision was deflected by two pledgeted sutures which were placed at each pole. After mitral procedure was completed, the left atrial roof was closed primarily with a 3-0 prolene suture to the septum and then the septal incision was closed using another 3-0 prolene suture, starting from the inferior pole of this incision. The air was evacuated from the left side and the aorta was unclamped. The right-sided procedure was carried out when required unclamping the aorta in most cases. The right atriotomy, then, was closed with a 4-0 prolene suture, starting from the two poles to the midpoint of the right atrial wall.
Left atrial approach
A superior venous cannula was inserted from the right atrial appendage, while an inferior venous cannula was inserted from the inferior vena cava. The procedure was performed between the confluence of the right pulmonary veins and the interatrial groove.
Data collection and postoperative patient management
Demographic characteristics of the patients, comorbidities, additional interventions such as coronary artery bypass grafting (CABG), De Vega's annuloplasty (DVA) for tricuspid regurgitation and ring annuloplasty, aortic repair, radiofrequency (RF) ablation, intraoperational data including cross-clamp time, mild hypothermia for myocardial protection, pre- and postoperative electrocardiographic (ECG) findings, postoperative complications including pacemaker implantation and increased bleeding and ischemia time were recorded.
Demographic and clinical characteristics of the patients were collected for both groups at the baseline. During surgery, cross-clamp and CPB time, antegrade arrest/prevention, inotropic support and duration of inotropic use were recorded. The amount of bleeding, need for cardiopulmonary resuscitation (CPR), duration of intubation, the presence of a pacemaker, length of hospital and intensive care unit (ICU) stay, postoperative ECHO on the postoperative 6th day and death events were also recorded following surgery. Patients with post- extubation dyspnea received bronchodilators and mechanical or non-invasive mechanical ventilatory support such as continuous positive airway pressure (CPAP) due to low saturation level and/or decreased partial oxygen pressure.
Statistical analysis
A statistical analysis was performed using SPSS v12.0 software (SPSS Inc., Chicago, Illinois, USA). Descriptive statistics were to analyze the demographic characteristics of the patients. Numerical variables were expressed in mean, median, standard deviation, minimum and maximum values, whereas categorical variables were expressed in numbers and percentages. A P value of <0.05 was considered significant.
Either parametric or non-parametric statistical methods were used according to normal distribution of comparative variables. The Student's t-test was used for numerical variables. This test was also used to compare normally distributed variables between the groups, while the Mann Whitney U test was used to compare abnormally distributed variables. The Wilcoxon test was used to compare pre- and postoperative values. Cross-tabulation was created for categorical variables (Chi -square, Fisher's exact and McNemar test).
RESULTS
Of the patients, 39 were males and 52 were females. The mean age was 54.0±15.4 (range, 16 to 82) years. The mean duration of complaints was 1.5±1.1 (range, 0.5 to 10) years. A total of 86.7% (n=79) were in NYHA Class III, while 12 were in NYHA Class IV. A total of 34.1% had diabetes mellitus (DM), 68.1% had chronic obstructive pulmonary disease (COPD), and 11.0% had coronary artery disease (CAD). Demographic and clinical characteristics of the patients undergoing STA or conventional LA are summarized in Table 1.
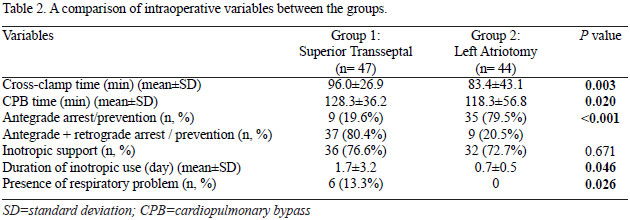
All patients had annuloplasty (42.9%) or valve replacement (57.1%). A total of 48.9% and 36.4% of the patients had annuloplasty in Group 1 and Group 2, respectively, whereas 51.1% and 63.6% of the patients had valve replacement in Group 1 and Group 2, respectively (P>0.05). Nineteen patients in Group 1 and 29 patients in Group 2 required additional interventions including CABG, DVA for tricuspid regurgitation, aortic repair, and RF ablation. Intraoperative data of both groups are summarized in Table 2. The mean diameter of the left atrium (LA) was 4.6±0.6 cm and 4.3±1.0 cm before and after STA, respectively, indicating a statistically significant difference (P<0.001). There was no statistically significant difference in pre- and postoperative diameters of LA between the groups.
Postoperative electrophysiological study findings
The mean pulmonary artery pressure (PAP) was 46.0±11.6 mmHg preoperatively and 37.0±9.4 mmHg postoperatively. The PAP values for each study group is shown in Table 3. A statistically significant difference in pre- and postoperative values was observed between Group 1 and Group 2 (P<0.001 and P=0.025, respectively).
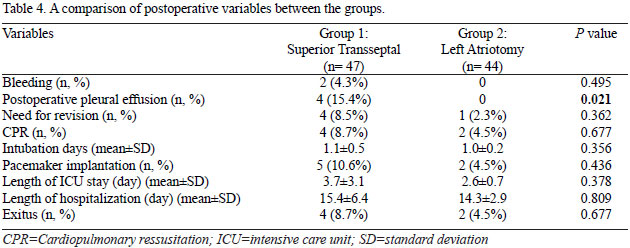
In preoperative and postoperative ECG studies, 78% and 74.2% patients were in sinus rhythm, while 22% and 22.5% had atrial fibrillation, respectively. There was no significant difference in pre- and postoperative ECG findings between the study groups. In Group 1, 32 of 36 patients who were in sinus rhythm preoperatively remained in sinus rhythm, 1 patient had atrial fibrillation, 2 patients were in nodal rhythm, and 1 had blocked rhythm after surgery. Out of 10 patients with preoperative atrial fibrillation, 3 were switched to sinus rhythm and 7 persisted in atrial fibrillation after surgery. In Group 2,25 of 33 patients who were in sinus rhythm before surgery remained in sinus rhythm, whereas 8 patients had atrial fibrillation postoperatively. Out of 10 patients with preoperative atrial fibrillation, 4 persisted in atrial fibrillation, whereas 6 were in sinus rhythm postoperatively (Figure 1). Change from baseline in the cardiac rhythm was statistically significant in STA group alone (P<0.001). Although clinical stages of the patients in Group 1 were more severe than those in Group 2 (patients in NYHA Class IV 25.5% vs. 0%, respectively), mortality rate was similar between the groups (8.7% vs. 4.5% respectively). A permanent pacemaker was implanted in 5 patients (10.6%) in Group 1, whereas in 2 patients (4.5%) in Group 2 (Table 4).

In the postoperative period, the mean ejection fraction (EF) values were 51.5 ± 14.4% in Group 1 and 40.1 ±12.9% in Group 2. There was a statistically significant difference in postoperative EF values between the groups (P<0.001). Pre- and postoperative mean ejection fractions were 57.2±9.9% and 51.5±14.4% in Group 1, respectively and 57.4±10.0% and 40.1±12.9% in Group 2, respectively. A statistically significant difference in the postoperative ejection fraction values was observed between the groups (P=0.001 and P<0.001 for Groups 1 and 2, respectively). Data are presented in percentages in Figure 2.

While there was no statistically significant difference in preoperative EF values between Group 1 and Group 2 (P=0.930), a statistically significant difference in post-operative values was observed between the groups (P<0.001) (Table 3). There was no change from baseline in the number of patients with EF 30-50% (n=13 patients). However, 6 of 29 patients in Group 2 had EF>50% after the operation, while 23 remained at the level of EF 30-50%.
Among all patients, pacemaker implantation was performed only in 7 (7.7%) patients, including 5 (10.6%) in Group 1 and 2 (4.5%) in Group 2. The difference between the groups was not statistically significant (P=0.436).
There was no statistical significance in bleeding, total length of hospital and ICU stay, the presence of low cardiac output syndrome between the groups. A total of 6 patients died; 4 of them were in the Group 1. There was no statistically significant difference in the mortality rate between the groups (Table 4).
DISCUSSION
Currently, a changing pattern of mitral valve surgery has been gradually evolving. While the incidence of rheumatic mitral disease has been reducing, there is an increasing demand for the correction of mitral insufficiency associated with or without coronary artery disease. These patients have usually small left atria and they are usually scheduled for the operation depending on the coronary artery anatomy, before the left atria have time to enlarge. Moreover, valve replacement surgery is mainly replaced by mitral reconstruction which is performed at earlier stages of the disease thanks to the sophisticated techniques available. Therefore, limited operation area which leads to poor visibility and prevents achieving a better exposure of the mitral valve and subvalvular apparatus during surgery has been one of the main considerations of cardiovascular surgeons.
The STA has been defined as one of new surgical approaches to overcome these problems without compromising treatment success. As cardiovasculars surgeons have increased their experiences in new approaches, they prefer superior transseptal incision for patients who are not in sinus rhythm or those with sinus rhythm for whom the surgeon thinks that technical advantages of the incision outweighs the risk of sinus rhythm loss. Similarly, our study results indicate that STA provides an excellent exposure without significant complications in mitral apparatus compared to the conventional LA.
The sinus node (SN) function and atrial vulnerability after surgery still remain as important considerations with the STA, since the technique involves transecting the SN artery as well as the anterior internodal conduction pathway. While there are a number of published studies in favor of STA in the literature[1-3,5,12,13], many studies reporting potential concerns regarding the SN dysfunction and atrial vulnerability during postoperative period are available[7,10,14,15]. In a study including 52 patients who underwent mitral valve surgery through STA, the authors reported that the number of the patients with sinus rhythm and atrial fibrillation were equal preoperatively. Eleven patients had transient atrial fibrillation or junctional rhythms for approximately 2 weeks postoperatively. After the mean follow-up period of 15±8 months (range, 2-25 months), 25 of 26 patients persisted in sinus rhythm, while 4 patients with preoperative atrial fibrillation showed sinus rhythm at the postoperative 6th month. It was reported that none of the patients required permanent pacemaker implantation due to symptomatic or latent bradycardia as assessed by Holter ECG at the median follow-up time period of 15 months[16].
In our study, we observed favorable changes in ECG results in Group 1, indicating a very low incidence of STA-induced permanent or serious damage, despite the conduction problems and atrial vulnerability in the postoperative period. Depending on our results, we concluded that undesired postoperative events might be decreased by a better operative area exposure, which could also decrease postoperative complications, and increase the success rate of STA. In addition, increasing professional experiences of surgeons and a better understanding of the conduction system at the sinoatrial node would improve pre- and postoperative evaluation process to decide the most appropriate approach considering the clinical presentation of the patient. In the literature, Lukac et al.[17] reported that STA remained an independent risk factor in their study with a large sample size, in which they compared STA with the left atrial method. However, our results indicated similar mortality rates as well as permanent pacemaker implantation between the groups. Thus, it did not increase fatal or permanent clinical outcomes.
Despite possible drawbacks including increased ischemia time, length of hospital stay, CPB, cross-clamp time, and increased bleeding related to the procedure, as previously mentioned, some authors reported no significant difference between the study groups[18,19]. In line with the literature, we observed no significant differences in the amount of bleeding, re-operation, and the length of hospital and ICU stay between the groups in our study. However, intraoperative data revealed that cross-clamp time, CPB time, duration of inotropic use, and respiratory problems were significantly increased in the STA group, compared to the conventional LA group without leading to any severe or unmanageable complications.
In our study, the cross-clamp time and CPB time were longer in STA group, as larger incisions were performed and the closure of the incision was performed in two layers as superior and septal. In addition, STA has been a newly used operation method in our clinic, which might also be another reason for prolonged time. When the additional procedures were reviewed, we concluded that tricuspid ring annuloplasty was most commonly performed in the STA group, whereas DVA was the leading method in the conventional LA group. As DVA is more rapidly performed, we believe it might contribute to significant differences between the procedures.
The STA group mainly consisted of patients in NYHA Class IV including one of them based on the preoperative extracorporeal membrane oxygenation (ECMO). We believe that preoperative demography and ECMO might significantly prolong the duration of inotropic use in STA group, compared to the conventional LA group. Poor baseline characteristics of the patients in STA group might also lead to increased incidence of postoperative respiratory problems. A higher amount of bleeding in STA group which was not statistically significant between the groups resulted in a higher incidence of pleural effusion. We think that pleural effusion might be another cause of respiratory problems in STA group.
Limitations
Our study has also some limitations. Firstly, a multi-center study designed for a larger sample size may provide more conclusive results for subgroup analyses in comparison of the two surgical approaches. Secondly, more detailed preoperative electophysiological studies such as sinus node recovery time (SNRT), sinoatrial conduction time, intraatrial mapping, and calculation of corrected QT dispersion for each patient may offer a better approximation of the SN function postoperatively for each patient and more detailed information regarding the individually-tailored treatment. This would help us for a better elimination of confounding factors while comparing different approaches, as well as improved postoperative evaluations of clinical outcomes.
CONCLUSION
Our study results suggest that STA does not increase the incidence of arrhythmia and/or fatal outcomes after mitral valve surgery even in patients with a worse clinical condition.
REFERENCES
1. Alfieri O, Sandrelli R, Pardini A, Fucci C, Zogno M, Ferrari M, et al. Optimal exposure of the mitral valve through an extended vertical transseptal approach. Eur J Cardiothorac Surg. 1991;5(6):294-8.
2. Berreklouw E, Ercan H, Schönberger JP. Combined superior-transseptal approach to the left atrium. Ann Thorac Surg. 1991;51(2):293-5. [MedLine]
3. Guiraudon GM, Ofiesh JG, Kaushik R. Extended vertical septal approach to the mitral valve. Ann Thorac Surg. 1992;52(5):1058-60.
4. Masiello P, Triumbari F, Leone R, Itri F, Del Negro G, Di Benedetto G. Extended vertical transseptal approach versus conventional left atriotomy for mitral valve surgery. J Heart Valve Dis. 1999;8(4):440-4. [MedLine]
5. Gaudino M, Alessandrini F, Glieca F, Martinelli L, Santarelli P, Bruno P, et al. Conventional left atrial versus superior septal approach for mitral valve replacement. Ann Thorac Surg.1997;63(4):1123-7. [MedLine]
6. Lukac P, Hjortdal VE, Pedersen AK, Mortensen PT, Jensen HK, Hansen PS. Atrial incision affects the incidence of atrial tachycardia after mitral valve surgery. Ann Thorac Surg. 2006;81(2):509-13. [MedLine]
7. Kumar N, Saad E, Prabhakar G, De Vol E, Duran CM. Extended transseptal versus conventional left atriotomy: early postoperative study. Ann Thorac Surg. 1995;60(2):426-30. [MedLine]
8. Takeshita M, Furuse A, Kotsuka Y, Kubota H. Sinus node function after mitral valve surgery via the transseptal superior approach. Eur J Cardiothorac Surg. 1997;12(3):341-4. [MedLine]
9. Tambeur L, Meyns B, Flameng W, Daenen W. Rhythm disturbances after mitral valve surgery: comparison between left atrial and extended trans-septal approach. Cardiovasc Surg. 1996;4(6):820-4. [MedLine]
10. Utley JR, Leyland SA, Nguyenduy T. Comparison of outcomes with three atrial incisions for mitral valve operations. Right lateral, superior septal, and transseptal. J Thorac Cardiovasc Surg. 1995;109(3):582-7. [MedLine]
11. ACC/AHA/ESC Guidelines for the Management of Patients With Atrial Fibrillation: Executive Summary A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for the Management of Patients With Atrial Fibrillation) Developed in Collaboration With the North American Society of Pacing and Electrophysiology. Circulation. 2001;104(17):2118-50. [MedLine]
12. Kon ND, Tucker WY, Mills SA, Lavender SW, Cordell AR. Mitral valve operation via an extended transseptal approach. Ann Thorac Surg. 1993;55(6):1413-6.
13. Masuda M, Tominaga R, Kawachi Y, Fukumura F, Morita S, Imoto Y; et al. Postoperative cardiac rhythms with superior-septal approach and lateral approach to the mitral valve. Ann Thorac Surg. 1996;62(4):1118-22. [MedLine]
14. Smith CR. Septal-superior exposure of the mitral valve. The transplant approach. J Thorac Cardiovasc Surg. 1992;103(4):623-8. [MedLine]
15. Arsiwala S, Parikh P, Dixit S, Agney M, Kole S, Saksena D. Combined superior-transseptal approach to the mitral valve. Ann Thorac Surg. 1992;53(1):180-1. [MedLine]
16. Misawa Y, Fuse K, Kawahito K, Saito T, Konishi H. Conduction disturbances after superior septal approach for mitral valve repair. Ann Thorac Surg. 1999;68(4):1262-4.
17. Lukac P, Hjortdal VE, Pedersen AK, Mortensen PT, Jensen HK, Hansen PS. Superior transseptal approach to mitral valve is associated with a higher need for pacemaker implantation than the left atrial approach. Ann Thorac Surg. 2007;83(1):77-82. [MedLine]
18. Nguyen HU. Improved combined superior-transseptal approach to the mitral valve. Asian Cardiovasc Thorac Ann. 2009;17(2):171-4. [MedLine]
19. García-Villarreal OA, Gonzáles-Oviedo R, Rodríquez-Gonzáles H, Martínez-Chapa HD. Superior septal approach for mitral valve surgery: a word of caution. Eur J Cardiothorac Surg. 2003;24(6):862-7. [MedLine]
No financial support. No conflict of interest
Authors' roles & responsibilities
EA: Planner, writer, drafting the study, collection, analysis and interprettion of data
AA: Collection, analysis and interpretation of data
MO: Study Design
Article receive on Wednesday, September 18, 2013
 All scientific articles published at rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at rbccv.org.br are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()


 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket