![]()
![]()
Tiago R. VelhoI; Nádia JunqueiraI; André SenaI; Hugo FerreiraI; Catarina CarvalheiroI; Nuno GuerraI; Javier GallegoI; Ângelo NobreI
DOI: 10.21470/1678-9741-2017-0044
INTRODUCTION
Melanoma is a tumor that arises from melanocytes or melanocyte precursors, and may virtually involve any tissue in the body[1]. It commonly metastasizes to the heart (40-45% of the cases)[1], but usually cardiac involvement is only diagnosed post-mortem because of the absent or nonspecific cardiac signs and symptoms[2]. Secondary cardiac lesions are up to 100 times more frequent than primary tumors[3]. Although they usually tend to remain silent[3], cardiac melanoma can cause serious mechanical (e.g. limitation of blood flow through the cardiac chambers) and electrical complications (usually associated with myocardial infiltrative masses) and embolization of the tumor[4]. In this article, we present a case of a patient admitted to the hospital with chest pain and diagnosis of myocardial infarction, with a ventricular mass identified. Histologic analysis after surgical resection revealed an occult metastatic melanoma.
CASE REPORT
A 41-year-old man without any cardiovascular risk factor presented to the emergency department with a 2-hour history of atypical chest pain. The patient had no history of previous episodes, or any other sign or symptom. At the examination, his pulse was arrhythmic at 125 beats/min. The electrocardiogram showed atrial fibrillation and 5 mm-ST-segment elevation on the inferior derivations. Troponin T was 3628 ng/L. The patient underwent immediate coronariography, and a thrombotic occlusion was visualized in the right coronary artery (Figure 1A), which was treated with aspiration, percutaneous balloon and abciximab (Figure 1B). The thrombus was not collected to histological analysis.
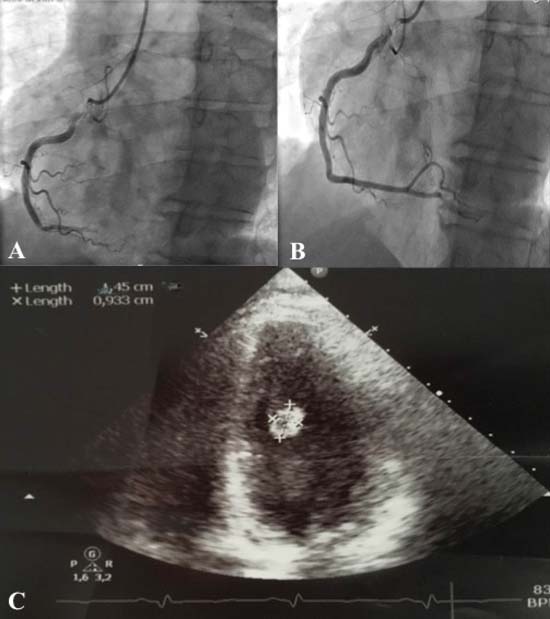

The echocardiogram showed hypokinesia of the inferior and posterior walls with normal left ventricular function, and the presence of a 10 x 15 mm mass (assumed to be a thrombus) adjacent to the mitral valve, causing mild to moderate mitral regurgitation (Figure 1C). The mass was unaltered with anticoagulation for 48 hours, so the patient was proposed to surgery. The patient was transferred to the cardiothoracic surgery department and was submitted to resection of the ventricular tumor. An 8 cm mini-thoracotomy was performed on the right 5th intercostal space and peripheral cannulation cardiopulmonary bypass was established. On the epicardial adipose tissue dark lesions were observed and excised for pathology. After left atriotomy, a large (2 x 2 cm), round and solid mass adjacent to the papillary muscle (Figure 2A) was causing mitral valve regurgitation. The mass was excised, including a partial resection of a papillary muscle, and sent for pathological examination. The mitral valve was surgically repaired with an annuloplasty (32 mm-ring) (Figure 2B). After annuloplasty, no regurgitation was observed during intraoperative echocardiogram.
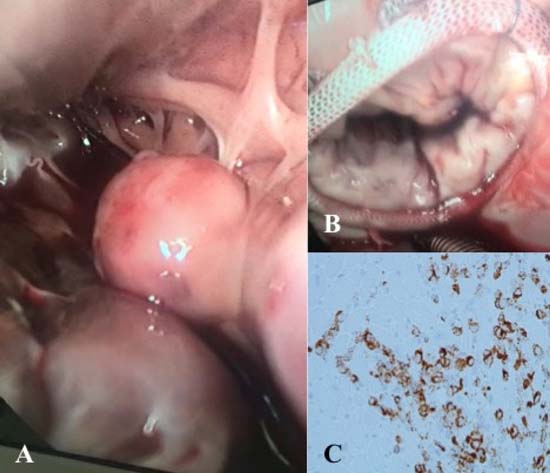

Pathological examination revealed that undifferentiated tumor cells infiltrated both the papillary muscle and epicardial adipose tissue. The tumor cells were positive on the immunocytochemistry to melan-A, vimentin, MITF and HMB45 (negative to CKAE1/AE3, CK7, CK20, LCA, CD3, CD20, WT1 and calretinin), concluding that the tumor was a melanoma (Figure 2C). The presence of the BRAF-V600E mutation was detected.
The patient's postoperative course was uneventful. He was discharged on the fourth postoperative day and referred to the oncology department. The patient underwent a thoraco-abdominopelvic computed tomography, which revealed metastatic disease to the lungs, liver, skin and lymph nodes. The patient started chemotherapy with vemurafenib and cobimetinib, to which he remains with partial response.
CONCLUSION
Although cardiac involvement in metastatic melanoma is frequent, symptomatic presentations are rare[2]. Most cases are not diagnosed antemortem due to the silent clinical course[4].
Most metastasis are located in the myocardium and valvular structures are typically unaffected[4]. When searching for a primary focus of the metastatic melanoma, mucosal (including genital mucosal) and ophthalmologic examinations are essential and must not be disregarded.
Few articles have been published reporting cardiac metastasis of malignant melanoma with unknown primary origin. In this case, the acute coronary syndrome was its first manifestation, since the patient had no history of previous mucosal and/or skin lesions or surgery.
We highlight the essential high level of suspicion, since cardiac tumors should raise the possibility of being a metastatic melanoma.
REFERENCES
1. Wick MR, Gru AA. Metastatic melanoma: pathologic characterization,current treatment, and complications of therapy. Semin Diagn Pathol.2016;33(4):204-18.
2. Allen BC, Mohammed TL, Tan CD, Miller DV, Williamson EE, Kirsch JS.Metastatic melanoma to the heart. Curr Probl Diagn Radiol.2012;41(5):159-64.
3. Auer J, Schmid J, Berent R, Niedermair M. Cardiac metastasis ofmalignant melanoma mimicking acute coronary syndrome. Eur Heart J.2012;33(5):676.
4. Basarici I, Demir I, Yilmaz H, Altekin RE. Obstructive metastaticmalignant melanoma of the heart: imminent pulmonary arterial occlusion caused byright ventricular metastasis with unknown origin of the primary tumor. HeartLung. 2006;35(5):351-4.
No financial support.
No conflict of interest.
Authors' roles & responsibilities
TRV Substantial contributions to the conception or design of the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
NJ Substantial contributions to the conception or design of the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
AS Substantial contributions to the conception or design of the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
HF Substantial contributions to the conception or design of the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
CC Substantial contributions to the conception or design of the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
NG Substantial contributions to the conception or design of the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
JG Substantial contributions to the conception or design of the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
AN Substantial contributions to the conception or design of the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
Article receive on Friday, April 21, 2017
 All scientific articles published at rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at rbccv.org.br are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()
 Read in English
Read in English
 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket