![]()
![]()
Minna Moreira Dias RomanoI; Antônio Carlos MenardiII; Osvaldo César Almeida-FilhoI; Walter Vilella de Andrade VicenteII; Paulo Roberto Barbosa EvoraII
DOI: 10.21470/1678-9741-2018-0615
DOVM = Double-orifice mitral valve
ASD = Atrial septal defect
TEE = Transesophageal echocardiogram
TTE = Transthoracic echocardiogram
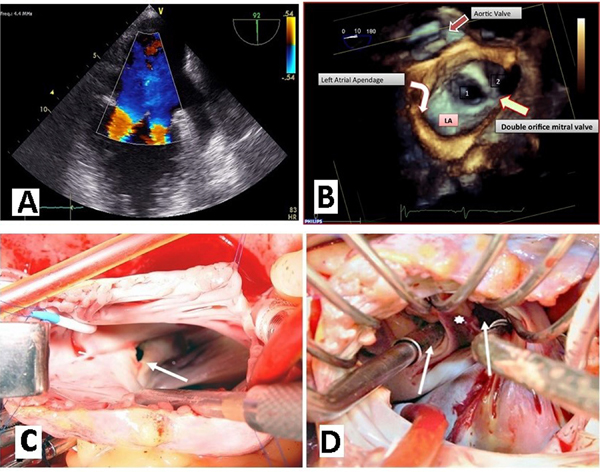

A 59-year-old male patient with history of aortic coarctation correction surgery at age 11 presented at the emergency room with severe inspiratory dyspnea and mitral systolic murmur. He was a patient without follow-up after surgical correction of aortic coarctation until the appearance of increasing dyspnea in the last 2 years. The first possible diagnosis of double-orifice mitral valve (DOVM) was based on echocardiogram data performed in 2012 as part of the investigation of increasing dyspnea. The recent transesophageal echocardiogram (TEE) revealed normal ventricular function, moderate to severe mitral regurgitation, DOMV and an 11-mm ostium secundum atrial septal defect (ASD).
Discussion of Questions
Double-orifice mitral valve is usually associated with other cardiac anomalies, so, it is supposed that DOMV is a congenital valve disease (Question A).
There are no specific clinical signs suggestive of DOMV. DOMV is usually an incidental finding in the diagnosis of the elderly patient and may be missed or undiagnosed in asymptomatic or even symptomatic patients. Most patients stay in normal sinus rhythm, but patients with significantly dysfunctional DOMV may present with heart failure, requiring initial medical therapy. The isolated cases of DOMV do not need therapy and can be followed up only by echocardiographic examinations. However, clinic manifestation and management depend not only on the severity of mitral valve dysfunction, but also on associated malformations, which cause pulmonary hypertension due to pulmonary hyperflow from intracardiac shunt (Question B).
Transthoracic echocardiogram, especially in parasternal short-axis views, is a reliable method and in most cases, sufficient to confirm a diagnosis of DOMV and to determine its type. 3D transthoracic echocardiogram is a diagnostic imaging method complementary to 2D transthoracic echocardiogram. Combining 2D and 3D transthoracic echocardiogram is extremely beneficial in the complete cardiac evaluation and management of DOMV (Question C).
In a severely stenotic DOMV, percutaneous balloon mitral valvuloplasty has been described, but the experience is limited. In most cases, the dividing bridge is composed of mitral and chordal tissue. Surgical transection of the dividing bridge is not advised in order to avoid iatrogenic mitral regurgitation. Therefore, a valve prosthesis is the most reliable surgical option (Question D).
Brief Consideration of the Case Reported
As the evaluation of dyspnea was mandatory for a possible surgery indication, the diagnosis was supplemented by ergospirometry and cardiac catheterization to better define the cause of dyspnea, clarified that the patient did not present pulmonary arteriolar hypertension and that pulmonary artery pressure was elevated by the presence of mitral valve insufficiency and ASD. Then the surgery was indicated. An atrial septostomy allows easy surgical access to the mitral valve apparatus that presented a duplicate mitral valve, with two separate mitral valve annuli, each with its own set of leaflets and subvalvular apparatus. It was implanted a 33M bovine pericardium prosthesis. Unfortunately, it was not possible to preserve the papillaries due to their irregular implantation. The immediate postoperative period was characterized by the difficulty of discontinuing respiratory care. The patient died after about 45 days, due to hospital pneumonia that evolved to septic shock[1-7].
Learning Points
• DOMV is usually discovered in childhood or early adolescence because of
its association with other congenital heart defects.
• The incidence of the diagnosis of DOMV in the adult tertiary referral
echocardiographic laboratory is 0.06%.
• DOMV is usually an incidental finding in the diagnosis of the elderly
patient, and’s diagnosis may be missed or undiagnosed in asymptomatic or
even symptomatic patients.
• DOMV as a cause of symptomatic mitral valve disease is also seen in
middle-aged/elderly people. Most patients remain in normal sinus
rhythm.
• TTE examination, especially in short-axis parasternal views, is a
reliable and, in most cases, sufficient method to confirm the diagnosis
of DOMV and to determine its type. However, three-dimensional TTE should
be used to better delineate and study the anomaly.
REFERENCES
1. Anwar AM, McGhie JS, Meijboom FJ, Ten Cate FJ. Double orifice mitralvalve by real-time three-dimensional echocardiography. Eur J Echocardiogr.2008;9(5):731-2. doi: 10.1093/ejechocard/jen149.
2. Liu S, Ren W, Ma C, Yang J. Congenital Double-Orifice Mitral Valvein Asymptomatic Patients. Int Heart J. 2018 Jan 27;59(1):213-215. doi:10.1536/ihj.17-033. [MedLine]
3. Pillai VV, Karunakaran J. Repair of Double Orifice Left AV Valve(DOLAVV) with Endocardial Cushion Defect in Adult. Braz J Cardiovasc Surg.2017;32(4):338-40. doi: 10.21470/1678-9741-2016-0034. [MedLine]
4. Pires N, Li W, Senior R, Khattar RS. Incidental finding of a doubleorifice mitral valve in an elderly patient: value of 3D imaging. Echo Res Pract.2017;4(3):K21-K24. doi: 10.1530/ERP-17-0023. [MedLine]
5. Samiei N, Dehghan H, Pourmojib M, Mohebbi A, Hosseini S, Rezaei Y.Isolated double-orifice mitral valve in a young girl. ARYA Atheroscler.2017;13(6):295-8. [MedLine]
6. Sinha SK, Mishra V, Singh K, Asif M, Sachan M, Kumar A, et al.Bi-Luminal Mitral Valve: Incidence, Clinical Features, Associated Anomaly andEchocardiographic Evaluation. J Clin Med Res. 2016Dec;8(12):893-898. [MedLine]
7. Tomita Y, Yasui H, Tominaga R. Mitral valve repair for isolateddoubleorificemitral valve with torn chordae. Ann Thorac Surg.1997;64(6):1831-4.
No financial support.
No conflict of interest.
Authors' roles & responsibilities
MMDR Substantial contributions to the conception or design of the work; final approval of the version to be published
ACM Substantial contributions to the conception or design of the work; final approval of the version to be published
OCAF Substantial contributions to the conception or design of the work; final approval of the version to be published
WVAV Substantial contributions to the conception or design of the work; final approval of the version to be published
PRBE Substantial contributions to the conception or design of the work; final approval of the version to be published
Article receive on Sunday, August 12, 2018
Article accepted on Thursday, August 30, 2018
 All scientific articles published at rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at rbccv.org.br are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()
 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket