![]()
![]()
Kaushalendra RathoreI
DOI: 10.21470/1678-9741-2021-0160
ABSTRACT
Aortic valve repair combined with root stabilization procedures have been reported to have reliable mid to long-term outcomes, and this is one of the reasons that various surgical units are accepting these techniques as an option in selected cases. Aortic valve replacement is a standard procedure with established results, but to master its techniques there is a major uphill learning curve. A brief communication is presented on the aortic valve repair focusing on the lesser discussed aspects like global variability of the pathology and outcomes, variable referral patterns, and effect of ethnicity.
AR = Aortic regurgitation
AS = Aortic stenosis
AV = Aortic valve
AVIATOR = Aortic Valve Insufficiency and ascending aorta Aneurysm InternATiOnal Registry
AVr = Aortic valve repair
AVR = Aortic valve replacement
BAV = Bicuspid aortic valve
CTD = Connective tissue disease
FAA = Functional aortic annulus
IE = Infective endocarditis
RHD = Rheumatic heart disease
SOV = Sinus of Valsalva
STJ = Sinotubular junction
SVD = Structural valve deterioration
TOE = Transoesophageal echocardiogram
VSD = Ventricular septal defect
INTRODUCTION
Aortic valvular disease is a global public health hazard, and aortic pathologies have significant presence in all demographic groups, with overall increase in the ageing population[1]. Severely diseased aortic valves (AVs) are best managed with surgical interventions, and available surgical options are replacement using mechanical or bioprosthetic valve, homograft, Ross procedure using pulmonary autograft, or aortic valve repair (AVr). Aortic valve replacement (AVR) is a well-established procedure with proven long-term outcomes, but patients are constantly exposed to the risk of anticoagulation-related bleeding, valve thrombosis, structural valve deterioration (SVD), pregnancy-related issues, and infections following prosthetic implantation[2]. Freedom from valve-related reoperation favoured mechanical valves for all age groups for fifteen years, except for patients aged > 60 years[3]. Similarly, fifteen-year freedom from the valve-related morbidity favoured biologic valves for all age groups, except in patients < 40 years of age at operation.
Interpretation of large contemporary literature reveals that bioprosthetic valves appeared to be favourable in patients on the basis of the lower incidence of valve-related morbidity, but they are associated with increased overall valve-related reoperations (the actual freedom from valve-related reoperation in patients between 51-60 years were 98.3% and 59.7% for the mechanical and bioprosthetic groups, respectively)[4]. Une et al.[5] have reported good durability of the Hancock II aortic bioprosthesis up to the 10-year follow-up following the implantation in young patients (91.4% actuarial freedom from re-AVR due to SVD)[5]. Their series showed that SVD significantly increased from 10 years to 20 years after surgery, especially in patients aged < 50 years and, at the 20-year follow-up, actuarial freedom from re-AVR due to SVD was 41.4% in patients aged 50-59 years.
To reduce disadvantages of the bioprosthesis in the younger population, surgical community progressed towards the repairing options. It was surely influenced by the success of the mitral valve repair that AV, ascending aorta, and aortic arch became the next field of interest in last couple of decades. Pioneers like Yacoub, Davids, and El Khoury et al. have described various repair techniques with good long-term outcomes, which completely revolutionized aortic surgery and helped in developing it as a subspecialty[6-8]. With all supporting contemporary literature, a larger question still remains about its applicability, acceptance, and generalization of the indications, as the reoperation rate, even in high-volume centres, following AVr is approximately 10.23% within four years of follow-up[8].
COMMENTS
What is Driving AVr?
It is well stated that AVR with bioprostheses in young adults is associated with high rates of SVD and reintervention; in patients aged between 20 to 40 years, one or more reinterventions during their lifetime are anticipated[9]. Although early mortality is low, the long-term survival is reduced, with a life expectancy of 60% to 75% of the age- and sex-matched life expectancy of general population. Etnel et al.[9] have reported that bioprosthetic AVR in young adults is associated with low early mortality (3.30%), but the late mortality is high (2.39%/year), and thus overall life expectancy is impaired compared with the general population. Their study showed that thromboembolism (0.53%/year) and bleeding (0.22%/year) rates are far lower than reported for mechanical AVR in young adults (0.90%/year and 0.85%/year, respectively). Others have also reported that after AVR, thromboembolism and bleeding rates were higher compared to the general population and higher than after the Ross procedure and AVr[10]. On the other side, AVr is consistently associated with a low risk of late valve-related morbidity, thromboembolism (< 0.7%/patient year), bleeding (< 0.3%/patient year), and infective endocarditis (< 0.2%/patient year)[7,11]. Overall freedom from reoperation was 95% for tricuspid valves at 10 and 15 years, 89% for bicuspid aortic valves (BAV) at 10 years, and 83% for BAV at 15 years. These results are encouraging for a more widespread use of AVr, but undeniable factors like case selection and institutional case volume make a significant difference in the long-term outcomes.
Why is AVr Challenging?
AV is considered one of the parts of several components of the aortic root functioning unit and to achieve good repair outcomes, the surgeon has to address lesions at multiple levels, e.g., sinotubular junction (STJ), functional aortic annulus (FAA), sinus of Valsalva (SOV), and AV simultaneously (Table 1). In the initial experience, only FAA was in focus, and leaflet issues were remained unaddressed, but as experience grew, surgical groups identified the importance of leaflets, SOV, and the role of valvular pathology, respectively[12]. Basic concept of good repair is to increase free margin length with maximising coaptation height, and performing all these additional procedures not only increases myocardial ischemic time but also increases chances of repair failure[13].
| AR types | Aortic valve stenosis | Aortic root dilatation | STJ dilatation | SOV | Ascending aorta | Aortic arch | Surgical options | |||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | ||||||||
| RHD | Y | Common | Not common | Not common | No | No | No | AVR, AVr | ||
| BAV | Y | 85% of the cases | 15% of the cases | Y | Y | Y | Y | AVR, AVr with or without reimplantation (Davids), remodeling | ||
| CTD | Y | Y | No | Common | Y | Y | Y | Y | AVR, AVr with or without reimplantation (Davids) | |
| IE | Y | Not common | Possible | Possible | Possible | No | No | AVR | ||
| Degenerative | Y | Common | No | No | Possible | No | No | AVR | ||
| Congenital VSD | Y | No | No | No | No | No | No | AVr | ||
| Unicuspid valve | Y | Possible | Possible | Possible | Y | Y | AVR, AVr with or without reimplantation (Davids) | |||
AR=aortic regurgitation; AVr=aortic valve repair; AVR=aortic valve replacement; BAV=bicuspid aortic valve; CTD=connective tissue disease; IE=infective endocarditis; RHD=rheumatic heart disease; SOV=sinus of Valsalva; STJ=sinotubular junction; VSD=ventricular septal defect; Y=yes

In vast majority of the developing nations of southeast Asia, South America, and Africa, rheumatic heart disease (RHD) is still the most common valvular pathology, and mitral valve involvement is the most common finding, followed by multivalvular lesions[1]. While in the developed Western world, RHD numbers are going down with increase in the degenerative valvular lesions (30-50%), and more often degenerative valves are stenotic lesions. Although the overall incidence of connective tissue disorder and congenital AV disease is stable (25-40%), the numbers of pure aortic regurgitation (AR) are limited, which could be a bottleneck in the learning curve for the surgeons[14].
Another very important aspect of the reliable AVr is to recognise intraoperative etiopathology comprehensively and to standardise findings for the proper reporting. AR has been classified in three groups to help the pathophysiology of the lesion and decide about type of repair (Figure 1)[15]. In a retrospective surgical study, pure valvular AR (type 1 lesion) was reported in 46% of the cases, while 54% of the patients had annular or ascending aortic dilatation (types 2 and 3 lesion)[14]. AVr outcomes are better in types 1 and 2 regurgitant lesions, while type 3 AR had poor outcomes because of poor tissue quality. Normal range of coaptation height is between 4-5 mm, while geometric height and effective height are 5 mm (BAV) and 9 mm, respectively[15]. All these finer technical points are part of a long learning curve, and if AVr is not performed regularly, then results might be suboptimum.


Anaesthetic experience in the intraoperative transoesophageal echocardiogram (TOE) is pivotal during AVr or aortic root procedures (remodeling or reimplantation) as it can guide towards better functional repair. De Waroux et al. have predicted “repairability” on the TOE and reported high reoperation rates (35% at the four-year follow-up) after AVr in the high-risk valve anatomy (type 3 lesions, type 2 lesion with severe prolapse, moderate calcification, significant leaflet restriction, valve coaptation < 4 mm, coaptation below the annular plane, and need for large pericardial patch extension)[16].
Bicuspid Aortic Valve
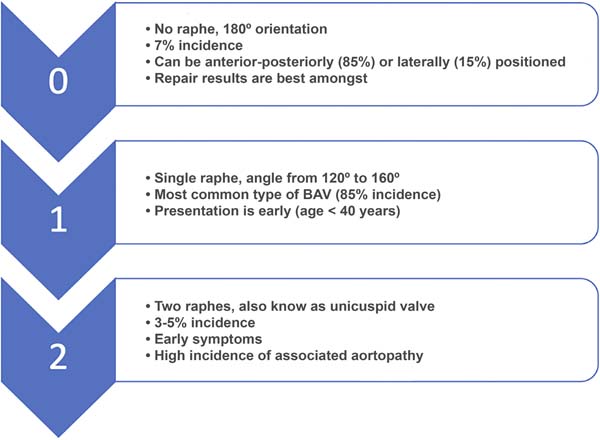
Cusp morphology in the BAV can be heterogeneous, and Sievers et al. have used a practical classification to report BAV valves[17]. BAV prevalence is in the range of 1%-2% in the general population (Figure 2). Type 0 BAVs are less common, have two symmetric aortic sinuses (180 degrees) with two commissures, and do not contain a median raphe. The two most common patterns of cusp fusion in type 0 BAV disease are fusion of the left and right coronary cusps, which occurs in 70%-85% of cases, and fusion of the right and noncoronary cusps, which occurs in 15%-30% of patients with BAV. The mechanism of AR in this most commonly BAV with two cusps, two sinuses, and two commissures at approximately 180 degrees (type 0) is ideal for the AVr[18]. In these patients, usually the prolapse of one or both cusps and the dilatation of the FAA is the cause of AR (type 2 lesion).
The more prevalent type 1 BAVs have a median raphe on the conjoint cusp and an asymmetric distribution of the aortic sinuses, with a large aortic sinus accompanying a large nonconjoint cusp and two smaller cusps fused together with a median raphe. AR in type 1 valves can be due to a rigid and restrictive raphe associated with smaller fused cusps (type 3 lesion). Mostly, BAVs are associated with aortic stenosis (AS) (85%) and in only 15% of the cases, aortopathy (dilated STJ and ascending aorta) is seen. Incidence of pure valvular AR is not well reported, although often it is caused by the annular or ascending aortic dilatation[19]. Aortopathy phenotype patients are mostly male, and they present early with the symptoms. Freedom from late adverse ascending aortic events in the operated patients of AR associated with BAV has poor prognosis compared to the AS with BAV (93±3% vs. 78±9% at 15 years postoperatively, respectively)[20].
Rheumatic Heart Disease
Mostly, type 1 and 2 lesions had better outcomes compared to RHD patients where major lesions are restriction and fibrosis[13]. Long-term outcomes of RHD valve repair are suboptimum and associated with high rate of reoperations[21]. Boodhwani et al.[22] have reported a five-year survival of 95% and freedom from reoperation of 92% in type 1 and 2 lesions. However, freedom from reoperation was reduced in restricted (type 3) groups (88% vs. 94% in types 1 and 2).
In a series from India, results of the rheumatic AVr have been presented using various repair techniques, and the reported freedom from the moderate to severe AV disease was 82.5% at eight years and 52.5% at 13 years of follow-up.
Various repair techniques have been described for AVr (peeling, shaving, extension, decalcification, free edge plication, commissurotomy, and neo-cuspidization), and often they are reasonable in mild to moderately damaged valves, but results are poor in severely affected lesions[23,24]. Ozaki et al.[25] have described a technique of leaflet neo-cuspidization using autologous pericardium and reported actuarial freedom from death, cumulative incidence of reoperation, and recurrence of the moderate AR as 85.9%, 4.2%, and 7.3%, respectively, at 54 months of follow-up. Ozaki technique can be an important method to create neo-leaflets in younger rheumatic patients where AVR might not be the best option. Various other groups have used this technique with few modifications and reported good mid-term to long-term outcomes[26]. Again, these highly specialized techniques will be hard to generalize for every cardiac unit and might lead to poor outcomes in the mid-term follow-up.
Does Aortopathy Differs in Caucasian vs. Non-Caucasian Population?
Multiple meta-analysis has demonstrated potential long-term benefit of valve-sparing root replacement in cases of aortopathy in Caucasian patients, but on the contrary, long-term follow-up in Asian population are limited and occasional[27,28].
The pattern of aortopathy in European and Asian population is significantly different as far as clinical features of the cardiovascular, ocular, and skeletal systems are concerned[29]. Asian Marfan populations have a higher prevalence of aortic root dilatation and mitral valve prolapse compared with Caucasian Marfan populations. Type 0 BAV was more frequently observed among Europeans compared with Asians (14.5% vs. 6.8%), whereas type 1 BAV with fusion raphe between the right and non-coronary cusps was more frequently observed in the Asian group compared with the European group (19.7% vs. 13.6%). In addition, the European group had higher prevalence of significant AR and diffusely dilated type of bicuspid aortopathy compared with the Asian group[30].
Another North American study showed that aortic dilatation and severity of BAV were higher in the Caucasian communities compared to the African American patients[31]. Their findings raise some important issues regarding the role of genetic, ethnic, or other vascular modifiers which need to be studied in the future. Russo et al.[32] have reported that patients who underwent surgery for type 1 BAV had more fibrosis, medio-necrosis, cystic medial necrosis, smooth muscle cell orientation, elastic fragmentation, and inflammation compared with other configurations in the follow-up.
It would be interesting to report differences in the aortopathy patterns from the different parts of the world and tailor-making surgical options based on those findings.
How Common is Pure AR and How Many Cases Surgeons Need to Keep Competence?
The Global Burden of Disease study group had reported that isolated AS was the third, and pure AR was the fourth most common valve lesion in RHD cases[33]. Even in the Western world, referral for pure AR is not frequent in the regular cardiothoracic units, and it significantly reduces surgical team’s competency in giving standard expected outcomes.
Malas et al.[34] have conducted a collaborative study with contribution from two busy AVr centres (one in Canada and another in Belgium) and reported about the learning curve to master the AVr technique. It takes approximately 40-60 cases to bring down complication rates, cardiopulmonary bypass time, aortic cross-clamping time, and to give standard reproducible outcomes. If surgeons are not getting regular referral, then they might take five to six years to perform the required numbers to overcome the steep learning curve.
Standardization of AVr Reporting
Standardization of the reporting can be tedious because of various surgical strategies, different techniques, and variable reporting patterns of the results[15]. Comparing outcomes with proven technique like AVR can be challenging[11]. The Aortic Valve Insufficiency and ascending aorta Aneurysm InternATiOnal Registry (AVIATOR) was created in European centres for enrolling patients with this subset of pathology[35]. The reconstructive surgery includes isolated valve repair in 27%, partial root or tubular aorta replacement plus valve repair in 23%, and valve-sparing root replacements in 50% of the cases. Replacements include isolated valve replacement in 22%, tubular aorta plus AVR in 19%, and root plus valve replacement (Bentall) in 59% of the cases. Most of the expert European centres on AVr are reporting patients in the AVIATOR, while participation from American (9.5%) and Asian countries is low (0.5%), which again reflects on the discord in reporting.
Follow-up and Reoperation
A multivariate analysis of the AVr failure in a series with 10-year follow-up using intraoperative TOE had identified a shorter coaptation length (< 4 mm), eccentric jet, coaptation occurring below the level of the aortic annulus, a larger aortic annulus, and residual AR (central jet > 3mm) at the end of surgery as high-risk factors of repair failure[36]. Type 3 repairs were especially at risk of AR recurrence because the leaflet tissue is either of not good quality (infective endocarditis, calcification, or rheumatic disease leading to the fibrosis) or insufficient to reconstruct the leaflet and require pericardial patching. Finally, another well reported pathological finding is the extension of native disease process in the residual repaired valve tissues and involves neo-cusp pericardial patch as well, eventually leading to AVr failure.
CONCLUSION
AVr is a leap forward step in the treatment of AV and root pathology but requires a careful team-approach in the decision making and execution. The surgical community requires further long-term reports from various demographic regions of the world before generalizing the indications. Number of cases and associated learning curve is well-established with these techniques, which reinforces the need for regular referrals to specific centres and can expand surgical experience in handling the complication-associated failures and help in developing AVr as a subspecialty.
REFERENCES
1. Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368(9540):1005-11. doi:10.1016/S0140-6736(06)69208-8. [MedLine]
2. Hammermeister K, Sethi GK, Henderson WG, Grover FL, Oprian C, Rahimtoola SH. Outcomes 15 years after valve replacement with a mechanical versus a bioprosthetic valve: final report of the veterans affairs randomized trial. J Am Coll Cardiol. 2000;36(4):1152-8. doi:10.1016/s0735-1097(00)00834-2. [MedLine]
3. Chan V, Jamieson WR, Germann E, Chan F, Miyagishima RT, Burr LH, et al. Performance of bioprostheses and mechanical prostheses assessed by composites of valve-related complications to 15 years after aortic valve replacement. J Thorac Cardiovasc Surg. 2006;131(6):1267-73. doi:10.1016/j.jtcvs.2005.11.052. [MedLine]
4. Jamieson WR, Burr LH, Miyagishima RT, Janusz MT, Fradet GJ, Ling H, et al. Re-operation for bioprosthetic aortic structural failure - risk assessment. Eur J Cardiothorac Surg. 2003;24(6):873-8. doi:10.1016/s1010-7940(03)00566-9. [MedLine]
5. Une D, Ruel M, David TE. Twenty-year durability of the aortic hancock II bioprosthesis in young patients: is it durable enough? Eur J Cardiothorac Surg. 2014;46(5):825-30. doi:10.1093/ejcts/ezu014. [MedLine]
6. Yacoub MH, Gehle P, Chandrasekaran V, Birks EJ, Child A, Radley-Smith R. Late results of a valve-preserving operation in patients with aneurysms of the ascending aorta and root. J Thorac Cardiovasc Surg. 1998;115(5):1080-90. doi:10.1016/S0022-5223(98)70408-8. [MedLine]
7. David TE, Feindel CM, Webb GD, Colman JM, Armstrong S, Maganti M. Long-term results of aortic valve-sparing operations for aortic root aneurysm. J Thorac Cardiovasc Surg. 2006;132(2):347-54. doi:10.1016/j.jtcvs.2006.03.053. [MedLine]
8. Boodhwani M, de Kerchove L, Glineur D, Poncelet A, Rubay J, Astarci P, et al. Repair-oriented classification of aortic insufficiency: impact on surgical techniques and clinical outcomes. J Thorac Cardiovasc Surg. 2009;137(2):286-94. doi:10.1016/j.jtcvs.2008.08.054. [MedLine]
9. Etnel JRG, Grashuis P, Huygens SA, Pekbay B, Papageorgiou G, Helbing WA, et al. The Ross procedure: a systematic review, metaanalysis, and microsimulation. Circ Cardiovasc Qual Outcomes. 2018;11(12):e004748. doi:10.1161/CIRCOUTCOMES.118.004748.
10. Etnel JRG, Huygens SA, Grashuis P, Pekbay B, Papageorgiou G, Roos Hesselink JW, et al. Bioprosthetic aortic valve replacement in nonelderly adults: a systematic review, metaanalysis, microsimulation. Circ Cardiovasc Qual Outcomes. 2019;12(2):e005481. doi:10.1161/CIRCOUTCOMES.118.005481.
11. Fok M, Shaw M, Sancho E, Abello D, Bashir M. Aortic valve repair: a systematic review and meta-analysis of published literature. Aorta (Stamford). 2014;2(1):10-21. doi:10.12945/j.aorta.2014.14-003.
12. Burt BM, ElBardissi AW, Huckman RS, Cohn LH, Cevasco MW, Rawn JD, et al. Influence of experience and the surgical learning curve on long-term patient outcomes in cardiac surgery. J Thorac Cardiovasc Surg. 2015;150(5):1061-7, 1068.e1-3. doi:10.1016/j. jtcvs.2015.07.068.
13. El Khoury G, de Kerchove L. Principles of aortic valve repair. J Thorac Cardiovasc Surg. 2013;145(3 Suppl):S26-9. doi:10.1016/j. jtcvs.2012.11.071.
14. Roberts WC, Ko JM, Moore TR, Jones WH 3rd. Causes of pure aortic regurgitation in patients having isolated aortic valve replacement at a single US tertiary hospital (1993 to 2005). Circulation. 2006;114(5):422-9. doi:10.1161/CIRCULATIONAHA.106.622761.
15. Lansac E, de Kerchove L. Aortic valve repair techniques: state of the art. Eur J Cardiothorac Surg. 2018;53(6):1101-7. doi:10.1093/ejcts/ ezy176.
16. le Polain de Waroux JB, Pouleur AC, Goffinet C, Vancraeynest D, Van Dyck M, Robert A, et al. Functional anatomy of aortic regurgitation: accuracy, prediction of surgical repairability, and outcome implications of transesophageal echocardiography. Circulation. 2007;116(11 Suppl):I264-9. doi:10.1161/ CIRCULATIONAHA.106.680074.
17. Sievers HH, Schmidtke C. A classification system for the bicuspid aortic valve from 304 surgical specimens. J Thorac Cardiovasc Surg. 2007;133(5):1226-33. doi:10.1016/j.jtcvs.2007.01.039.
18. David TE. Aortic valve sparing in different aortic valve and aortic root conditions. J Am Coll Cardiol. 2016;68(6):654-64. doi:10.1016/j. jacc.2016.04.062.
19. Girdauskas E, Borger MA. Bicuspid aortic valve and associated aortopathy: an update. Semin Thorac Cardiovasc Surg. 2013;25(4):310-6. doi:10.1053/j.semtcvs.2014.01.004.
20. Girdauskas E, Disha K, Secknus M, Borger M, Kuntze T. Increased risk of late aortic events after isolated aortic valve replacement in patients with bicuspid aortic valve insufficiency versus stenosis. J Cardiovasc Surg (Torino). 2013;54(5):653-9.
21. Myers PO, Tissot C, Christenson JT, Cikirikcioglu M, Aggoun Y, Kalangos A. Aortic valve repair by cusp extension for rheumatic aortic insufficiency in children: long-term results and impact of extension material. J Thorac Cardiovasc Surg. 2010;140(4):836-44. doi:10.1016/j.jtcvs.2010.06.036.
22. Boodhwani M, El Khoury G. Aortic Valve Repair. Oper Tech Thorac Cardiovasc Surg. 2009;14(4):266-80.
23. Talwar S, Saikrishna C, Saxena A, Kumar AS. Aortic valve repair for rheumatic aortic valve disease. Ann Thorac Surg. 2005;79(6):1921- 5. doi:10.1016/j.athoracsur.2004.11.042.
24. Afifi A, Hosny H, Yacoub M. Rheumatic aortic valve disease-when and who to repair? Ann Cardiothorac Surg. 2019;8(3):383-9. doi:10.21037/acs.2019.05.01.
25. Ozaki S, Kawase I, Yamashita H, Uchida S, Takatoh M, Kiyohara N. Midterm outcomes after aortic valve neocuspidization with glutaraldehyde-treated autologous pericardium. J Thorac Cardiovasc Surg. 2018;155(6):2379-87. doi:10.1016/j. jtcvs.2018.01.087.
26. Sá MPBO, Perazzo ÁM, Zhigalov K, Komarov R, Kadyraliev B, Enginoev S, et al. Aortic valve neocuspidization with glutaraldehydetreated autologous pericardium (Ozaki procedure) - a promising surgical technique. Braz J Cardiovasc Surg. 2019;34(5):610-4. doi:10.21470/1678-9741-2019-0304.
27. Flynn CD, Tian DH, Wilson-Smith A, David T, Matalanis G, Misfeld M, et al. Systematic review and meta-analysis of surgical outcomes in Marfan patients undergoing aortic root surgery by compositevalve graft or valve sparing root replacement. Ann Cardiothorac Surg. 2017;6(6):570-81. doi:10.21037/acs.2017.11.06.
28. Arimura S, Seki M, Sasaki K, Takai H, Matsuhama M, Kunihara T, et al. A nationwide survey of aortic valve surgery in Japan: current status of valve preservation in cases with aortic regurgitation. Gen Thorac Cardiovasc Surg. 2017;65(8):429-34. doi:10.1007/s11748-017-0795- 8.
29. Franken R, den Hartog AW, van de Riet L, Timmermans J, Scholte AJ, van den Berg MP, et al. Clinical features differ substantially between Caucasian and Asian populations of Marfan syndrome. Circ J. 2013;77(11):2793-8. doi:10.1253/circj.cj-13-0584.
30. Yoon SH, Ohno Y, Araki M, Barbanti M, Lin MS, Ahn JM, et al. Comparison of aortic root anatomy and calcification distribution between Asian and Caucasian patients who underwent transcatheter aortic valve implantation. Am J Cardiol. 2015;116(10):1566-73. doi:10.1016/j.amjcard.2015.08.021.
31. Chandra S, Lang RM, Nicolarsen J, Gayat E, Spencer KT, Mor-Avi V, et al. Bicuspid aortic valve: inter-racial difference in frequency and aortic dimensions. JACC Cardiovasc Imaging. 2012;5(10):981-9. doi:10.1016/j.jcmg.2012.07.008.
32. Russo CF, Cannata A, Lanfranconi M, Vitali E, Garatti A, Bonacina E. Is aortic wall degeneration related to bicuspid aortic valve anatomy in patients with valvular disease? J Thorac Cardiovasc Surg. 2008;136(4):937-42. doi:10.1016/j.jtcvs.2007.11.072.
33. Watkins DA, Johnson CO, Colquhoun SM, Karthikeyan G, Beaton A, Bukhman G, et al. Global, regional, and national burden of rheumatic heart disease, 1990-2015. N Engl J Med. 2017;377(8):713- 22. doi:10.1056/NEJMoa1603693.
34. Malas T, Saczkowski R, Sohmer B, Ruel M, Mesana T, de Kerchove L, et al. Is aortic valve repair reproducible? analysis of the learning curve for aortic valve repair. Can J Cardiol. 2015;31(12):1497.e15-22. doi:10.1016/j.cjca.2015.05.016.
35. de Heer F, Lansac E, El-Hamamsy I, Pibarot P, De Kerchove L, El Khoury G, et al. The AVIATOR registry: the importance of evaluating long-term patient outcomes. Ann Cardiothorac Surg. 2019;8(3):393-5. doi:10.21037/acs.2019.04.08.
36. le Polain de Waroux JB, Pouleur AC, Robert A, Pasquet A, Gerber BL, et al. Mechanisms of recurrent aortic regurgitation after aortic valve repair: predictive value of intraoperative transesophageal echocardiography. JACC Cardiovasc Imaging. 2009;2(8):931-9. doi:10.1016/j.jcmg.2009.04.013.
Authors’Roles & Responsibilities
KR Substantial contributions to the conception or design of the work; final approval of the version to be published
Article receive on Saturday, March 13, 2021
Article accepted on Saturday, May 15, 2021
 All scientific articles published at rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at rbccv.org.br are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()

 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket