![]()
![]()
Bruna EibelI; Clarissa G. RodriguesII; Imarilde I. GiustiI; Ivo A. NesrallaIII; Paulo R. L. PratesIII; Roberto T. Sant'AnnaIV; Nance B. NardiV; Renato A. K. KalilVI
DOI: 10.5935/1678-9741.20110056
ABSTRACT
Severe ischemic heart disease with refractory angina, occurs in increasing incidence. Alternative forms of treatment, in an attempt to reduce myocardial ischemia and relief of symptoms has been studied. In this context, gene therapy is an option, for the possibility of inducing angiogenesis, establish collateral circulation and reperfuse ischemic myocardium. Several clinical trials have been conducted and, except for specific cases of adverse effects, there is indication of safety, feasibility and potential effectiveness of therapy. The clinical benefit, however, is not yet well established. In this article we review the clinical trials of gene therapy for patients with ischemic heart disease. The approach includes: (1) myocardial ischemia and angiogenesis on the pathophysiological aspects involved, (2) growth factors, dealing with specific aspects and justifying the use in cardiac patients with no option for conventional therapy, (3) controlled clinical trials, where a summary of the main studies involving gene therapy for severe ischemic heart disease is presented, (4) our experience, especially on preliminary results of the first gene therapy clinical trial in Brazil and (5) future prospects.
RESUMO
Cardiopatia isquêmica grave com angina refratária a formas convencionais de tratamento apresenta-se em uma crescente incidência. Para tratar angina refratária, terapias alternativas na tentativa de redução da isquemia miocárdica e alívio de sintomas têm sido estudadas. Neste contexto, a terapia gênica representa uma opção, pela possibilidade de induzir angiogênese, estabelecer circulação colateral e reperfundir miocárdio isquêmico. Diversos ensaios clínicos têm sido conduzidos e, com exceção de casos isolados e específicos de efeitos adversos, há indicação de segurança, viabilidade e potencial eficácia da terapia. O benefício clínico não está bem definido. Neste artigo, revisamos os ensaios clínicos que utilizaram terapia gênica para tratamento de pacientes cardiopatas isquêmicos. A abordagem inclui: (1) isquemia miocárdica e angiogênese, sobre os aspectos fisiopatológicos envolvidos; (2) fatores de crescimento, tratando sobre aspectos específicos e justificando a utilização em pacientes cardiopatas isquêmicos sem opções pela terapêutica convencional; (3) ensaios clínicos controlados, onde é apresentado um resumo dos principais estudos envolvendo terapia gênica para tratamento da cardiopatia isquêmica grave; (4) nossa experiência, especialmente sobre resultados preliminares do primeiro ensaio clínico de terapia gênica do Brasil e (5) perspectivas.
INTRODUCTION
It is estimated that cardiovascular disease (CVD) cause approximately 17 million deaths worldwide each year, with higher prevalence in developed countries [1]. CVD should be leaders in mortality in the developing world within the next decades, reaching epidemic levels [1]. Coronary artery disease (CAD) is a problem of increasing prevalence, especially in large cities and the populations of older age, its mortality is 80% of deaths from CVD [2,3]. Angina refractory to traditional forms of treatment in cardiology, including percutaneous and surgical revascularization and optimal drug therapy, represents up to 15% of all cases of angina [2]. According to statistics from the American Heart Association [3], the prevalence of refractory angina in the U.S. population is 4.6%, affecting 58% of patients with CAD and growing rapidly with increasing age. Despite advances in treatment modalities, it is estimated that the incidence of patients with refractory angina will increase in coming years [4,5], pointing to the need for new treatment options.
In this context, gene therapy could be an option, due to the potential to induce myocardial angiogenesis and establish collateral circulation [5]. Gene therapy can be defined as a set of techniques that allow the insertion and expression of a therapeutic gene in target cells that have some kind of disorder of genetic origin (not necessarily hereditary), enabling the correction of inappropriate gene products that cause diseases, therefore being an alternative for the treatment of diseases based on the transfer of genetic material [6-8]. Studies have tested the effects on ischemic heart disease patients using different growth factors, several doses, vectors and routes of administration. It can be emphasized the vascular endothelial growth factor (VEGF), a regulator of endothelial cells, which has the property of mediating angiogenesis during tissue repair [4].
The availability of vectors with tropism for the myocardium, capable of a long and stable protein expression [9], and the isolation of progenitor cells with regenerative and angiogenic potential [10] offers possibilities for development of therapy based on protection and regeneration of ischemic myocardium.
Although promising, the clinical effects on the myocardial vasculature provided by gene therapy remain to be clarified fully. The aim of this study is to review the clinical trials of gene therapy for the treatment of ischemic heart disease patients.
GENE THERAPY APPLIED TO ISCHEMIC CARDIOMYOPATHY
Myocardial Ischemia and Angiogenesis
In the pathophysiology of ischemic heart disease, two processes are involved: supply and demand of myocardial oxygen. Myocardial ischemia occurs when there is imbalance between supply and demand for oxygen. Two situations alter the oxygen supply to the myocardium, ischemia and hypoxia. In some conditions, the impairment of oxygen is secondary to decreased blood flow and in other situations, the increase in oxygen demand is the main responsible for myocardial ischemia [11].
Features of molecular biology and gene therapy have been developed for application in cardiovascular therapy, in situations where there are no options, or when these conventional methods have limitations. The main area of development of gene therapy in cardiology is the induction of myocardial angiogenesis with potential benefits in end-stage ischemic heart disease, after exhaustion of pharmacological, surgical and interventional resources using catheter, ie, in those refractory cases to all forms of treatment, where only the use of cardiac transplantation would be possible[4].
Angiogenesis, the formation of new vessels from existing endothelium of blood vessels, has an important role in embryonic development, tissue repair and progression of a variety of pathological processes [12,13]. Angiogenesis induced by administration of growth factors is intended to promote the formation of new blood vessels, capillaries and arterioles.
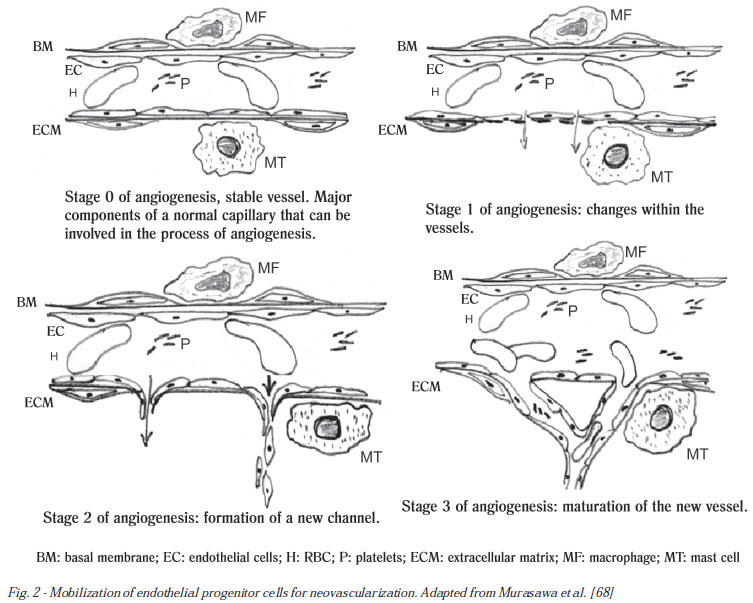
The mechanism of angiogenesis can be initiated by factors of a mechanical nature, by inflammatory or hypoxic process (energy imbalance). The process of angiogenesis occurs in stages (Figure 1) comprising: vessel dilation, endothelial cell activation, platelet activation, secretion of plasminogen activators and proteolytic enzymes, mast cell degranulation, activation of macrophages, disruption of the basement membrane and increased permeability with release of fibrin and other proteins. Following, formation of pseudopodia occurs, degradation of extracellular matrix, migration of endothelial cells to the extravascular space with the same proliferation and formation of shoots of vascular tissue. Finally, they form new basement membrane and maturation of the new establishment of the vascular wall to blood flow, formation of tubes and conections, establishing new vessels [14].
The idea that angiogenic factors may promote revascularization of ischemic tissues is called therapeutic angiogenesis [15]. The concept of therapeutic angiogenesis in humans through clinical trials phase I went ahead with the idea of testing this strategy in ischemic cardiomyopathy. Therefore, therapeutic angiogenesis is a strategy designed to amplify the natural process of angiogenesis and reperfuse ischemic tissues, which may represent a new process of revascularization in these high-risk patients [16].
There is a direct influence of inflammation and hypoxia on angiogenesis. Inflammation increases the production of PR-39macrophage-derived peptide, this inhibits the degradation of HIF-1α (hypoxia-inducible factor 1-α) leading to increased expression of VEGF and its receptors [17]. Inflammation induces the production of cytokines that promote angiogenesis [18]. In contrast, PR-39 increases the production of fibroblast growth factors (FGF), which have angiogenic power. Mechanical factors may act by activating the same mechanism, resulting in angiogenesis [10].
Vascular Endothelial Growth Factor, Fibroblast Growth Factor (FGF), hepatocyte growth factor (HGF) Plasmid and Aenoviral vector.
The formation of new blood vessels responds to the stimulation of angiogenic factors, which regulate endothelial migration, proliferation, survival, and proteolytic activity. Among the factors described in the literature, VEGF has emerged as a critical regulator of pro-angiogenic process [19-21]. This molecule promotes the formation of new vessels and their morphogenesis, through a complex process of angioregulatory events [22,23].
VEGF, family member of VEGF A, which consists of five isoforms resulting from alternative divisions of a single gene, ie, VEGF121, VEGF145, VEGF165, VEGF189 and VEGF206, is a growth factor specific to the endothelium [24.25 ]. It acts mainly by activating two Flt-1 tyrosine kinase receptors (fms-like tyrosine kinase-1, VEGF receptor-1) [26] and KDR (kinase-insert domain-containing receptor, VEGF receptor-2) [27] but can also activate other receptors, such as Neuropilins-1 and 2 [28]. VEGF may represent a new treatment modality for ischemic heart disease. This is due to the possibility of developing new blood vessels or promote the reformation of existing vessels [29]. The VEGF165 contains 165 amino acids and works by interacting with specific receptors on endothelial cells, initiating the cascade of events that culminates in endothelial cell migration, proliferation and aggregation of microtubules that will eventually form a network of arterial and venous systems.
Gene therapy in cardiovascular diseases is not intended to replace an abnormal gene, but suprarregular the expression of a useful protein, increasing DNA content. Its effectiveness depends on the gene vector and method of administration used [30]. VEGF functions both as an important marker of endothelial damage, as the mediator of repair. In cases of injury such as ischemia, inflammation and infarction have their expression increased. In addition, it encourages the maintenance, mobilization and recruitment of endothelial progenitor cells (EPC) from bone marrow [31]. The angiogenic potential of VEGF stimulates endothelial production of nitric oxide through activation of nitric oxide synthase (eNOS) (Figure 2).
The endothelium synthesizes important substances, playing a key role on the vascular control, both in physiological conditions and in pathological processes such as acute coronary syndromes. The monolayer of endothelial cells acts as a nonstick surface for platelets and leukocytes, producing a variety of important regulatory factors, such as NO [32]. Thus, influences not only vascular tone but also its remodeling through the production of substances promoting and inhibiting their growth [33].
Dysfunction in endothelial cells leads to a loss of antithrombotic properties of vascular wall and corresponds to the beginning of the atherosclerotic process [32]. The reconstruction occurs by endothelial migration and proliferation of circulating mature endothelial cells. However, these cells have low proliferative potential and their ability to repair is limited. Evidence indicates that peripheral blood contains bone marrow cell subsets, with properties similar to embryonic angioblastic. EPCs have a proliferative capacity and differentiate into mature endothelial cells, and can be induced by various cytokines or growth factors, acquiring different phenotypes [32].
The FGF family comprises at least nine polypeptides, including acidic FGF and basic FGF. Unlike VEGF, FGF acts in the mitogenesis of endothelial cells, fibroblasts and smooth muscle cells [18]. The increased availability of FGF provided the use of this gene has been most studied. Among the experimental studies, we highlight the report by Kawasuji et al. [34] in a model of acute myocardial infarction, where the response to FGF demonstrated to increase the number of capillaries in the border zone and in the epicardium of the infarcted area, the increased blood flow in these areas and the improvement in left ventricular ejection fraction 7 days after infarction.
On the other hand, HGF is a potent mitogen for a wide variety of cells, and angiogenic, antiapoptotic and possess antifibrotic properties [35,36]. In a pilot study of gene therapy in patients with CAD, Yang et al. [37] reported the growing evidence of the beneficial effects of HGF in myocardial infarction, heart failure and peripheral arterial disease. The aim of this study was to assess the effects of intracoronary administration of an adenovirus vector encoding the human HGF gene (Ad-HGF) on serum levels of cytokines and mobilization of CD34 (+) and CD117 (+) cells in patients with heart disease. Given the findings, it was concluded that gene therapy with HGF may play an important role in the regulation of inflammatory cytokines and induce mobilization of EPCs in patients with CAD.
Genetic vectors are all DNA molecules with potential for autonomic replication within the host cell in which DNA sequences can be inserted and expanded. The origin of the vector plasmid allows to classify in bacteriophage or viral infections [38]. They are used to transport genes into recipient cells. They have not only markers for ease of recognition as well as replicating sequences. Common vectors include plasmids carriers for transportation of naked DNA and viral vectors such as adenovirus, retrovirus and lentivirus.
Advantages and disadvantages compared to the vector used include the size of the inserted gene, the site of incorporation in the nucleus, the duration of expression, the transfer efficiency and the degree of body's immune response [39]. The plasmid vector is expressed by only a few days after viral vector administration and shows gene expression for several weeks [40]. Thus, the clinical studies that attempt to treat end-stage ischemic disease through gene therapy may be limited by duration of exposure to inadequate angiogenic agent [4].
Gene therapy suffered a major setback when the occurrence of death in a research subject, probably due to high viral load administered, and there was cancellation of several clinical projects and return to the laboratory research. Since 2000, few projects have been developed for clinical application. Theoretically, before being introduced into the patient, the viruses used as vectors suffer from several genetic changes, so that the therapeutic gene is inserted, while several other genes that confer virulence are removed or inactivated [7,41,42]. Thus, when binding and invading the target cell, the viral vectors inject its genetic material containing the therapeutic gene in the patient's DNA, allowing transcription and translation of the gene to their corresponding functional protein, or using the molecular machinery of the host cell to express their genes. However, in specific cases, the virulence became something uncontrollable, where the therapy became the cause of death of patients undergoing such intervention. On the other hand, plasmid vectors have no gene size limit to be inserted and induces minimal immune response, resulting in sustained transgenic expression. The disadvantage is the low rate of transfer of the encoding gene of the angiogenic factor [43].
The ideal vector would be one that combines low immunogenicity and a satisfactory safety profile, with high efficiency of transfection and transgene expression to specific time periods [4].
Gene transfer to the myocardium has been used as an alternative strategy to achieve a sustained local expression of angiogenic proteins [44]. There is a variety of different methods to replace or repair the genes targeted in gene therapy. A normal gene can be inserted into a nonspecific location within the genome to replace a nonfunctional gene, which is the most common approach, though, an abnormal gene could be replaced by a normal gene through homologous recombination, an abnormal gene could be repaired through selective reverse mutation, which returns the gene to its normal functions and also the regulation of a gene can be altered, such regulation corresponding to the degree to which a gene is active or inactive [6-8].
Controlled Clinical Trials of Gene Therapy
Despite more than a decade of achievement of the first clinical trial of gene therapy [45], the real clinical benefits of this therapy still need to be better elucidated. Research has attempted to identify other parameters and outcomes that can provide objective evidence of bioactivity and clinical improvement [4]. Thus, among the studies, it can be observed the use of different genes, doses, types of vectors and routes of administration. In Table 1, are gathered clinical trials involving gene therapy with VEGF with interventions performed via left minithoracotomy, in Table 2, studies using the percutaneous method, and in Table 3 are gathered clinical trials of gene therapy with FGF.
This study highlights the potential clinical applications of growth factors in humans, since experimental studies have shown favorable results and initial clinical studies in humans do not report adverse events related. Current tests report that the use of high doses of VEGF, compared with low doses and placebo, improves myocardial perfusion in patients with severe angina and provides evidence of a dose-dependent positive effect [46.47]. Confronted with evidence, VEGF has been shown to be a potential angiogenic factor, which benefits in medium and long term follow-up have been or are being assessed, including the improvement of quality of life, functional class of heart failure, angina class, functional capacity and reduction of myocardial ischemia [25,28,45,46,48-57].
FGF [58-60] and HGF [61] have also been demonstrating its potential benefits in the induction of myocardial angiogenesis, and to further develop this promising therapeutic approach we must critically assess the results and the experimental protocols, to identify factors that may have undermined the effectiveness of therapy or confounding data interpretation [4].
As the route of administration, the intramyocardial route proved to be more effective and, therefore, have been the most widely used in studies involving gene therapy in cardiology [38]. Previous studies suggest that administration by intramuscular injection offers the possibility to offer more effective in focal areas of ischemic muscle [4].
There are questions concerning the safe transfer of angiogenic factors, and also in relation to time of expression [4.62], where it is known that plasmids carriers of angiogenic factors protein, because they have more short expression and do not incorporate DNA to which the cell will connect to, have a lower risk of this adverse effect. Since the viral vectors require care in biosafety, it is unnecessary measure with non-viral vectors. Studies indicate temporary events related to use of adenovirus, such as fever or elevated serum C-reactive protein, liver enzymes and antibody titration [22]. Hao et al. [63] published in 2007, an experimental study on myocardial angiogenesis VEGF165 compared with adenoviral plasmid vector. These authors demonstrated equivalent benefits in terms of ventricular function (P<0.05) for plasmids and adenovirus after 4 weeks, however, in this study, the TUNEL technique that detects DNA breaks that occur during the process of apoptosis, demonstrated an increase in frequency of cardiomyocyte apoptosis in adenovirus group (P <0.02).
Almost all clinical trials of gene therapy and study population are patients with end stage ischemic disease, since the possible increased risk in relation to the benefits associated with new treatments are acceptable and can be used as an adjunct to conventional therapy. However, in very advanced clinical situations, therapy may not lead to an improvement of great intensity and measurable by available methods, even when treatment shows some clinical benefit [4.64].
Local Experience
In the Cardiology Institute of RS/FUC and the Discipline of Cardiology of UFCSPA, in collaboration with the Laboratory of Immunogenetics, UFRGS, we previously developed experimental studies [65-67] and recently performed the first gene therapy clinical trial in Brazil, using VEGF165 for refractory angina [53].
In experimental studies, we used a canine model of myocardial infarction in acute and chronic phases in an attempt to assess the processes of gene therapy. Recently, we developed a controlled clinical trial, phase I/II (ClinicalTrial NCT00744315) [53] in order to clinically assess the effects of gene therapy with VEGF165 in patients with advanced coronary artery disease (CAD), not eligible for revascularization or percutaneous surgical. The thirteen patients received optimal drug therapy for at least six months and underwent administration of intramyocardial injections of 2000 µg of plasmid VEGF165. Patients were assessed by myocardial scintigraphy, exercise testing, quality of life questionnaire (Minnesota) and determination of classes of heart failure (NYHA) and angina (CCS). In partial results of 3 months of evolution, it was concluded that the therapy proved to be safe and feasible, tending to improvement in severity of angina and reducing the intensity of myocardial ischemia.
CONCLUSIONS
Over 1,000 patients were enrolled in controlled clinical trials of gene therapy, covering more than a decade and so far, except for specific cases, no adverse safety signal was detected, indicating that the therapy is safe, feasible and potentially effective although they have not produced conclusive evidence of its benefits definitely. Reports of retinopathy, cancer or other diseases that could be driven by vascular growth were perceived as equally distributed in treated and placebo groups in randomized clinical trials.
More definite conclusions about risks and complications will require more follow-up time and number of patients undergoing therapy [4]. Thus, gene therapy has emerged as a potentially beneficial alternative to ischemic heart disease patients, when conventional therapies are exhausted. The definition of angiogenic success, for better assessment of the results needs to be rethought and defined by methods of higher sensitivity and specificity.
Traditionally, therapy for the treatment of cardiovascular disease should demonstrate improvements in morbidity and mortality. However, for this patient population, the fact of improving quality of life, and decrease or elimination of episodes of angina and reduction of events of hospitalization may be considered the biggest gains on this new therapy. Knowing that the manifestations of cardiovascular disease is progressive, the main aim is to offer patients significant decrease of symptoms and delay this progression.
The future directions of gene therapy indicate probable combinations of angiogenic factors or individual factors (HIF 1-α) that activate different pathways of neovascularization. Combinations of cell therapy and angiogenic factors, as well as the use of biomaterials to improve the microenvironment are other promising strategies for ischemic tissue repair [4].
ACKNOWLEDGEMENTS
The authors acknowledge the participation in group projects of Gene Therapy of the Institute of Cardiology of Rio Grande do Sul/University Foundation of Cardiology, toe following colleagues: Leonardo Karam Teixeira, Felipe Borsu de Salles, Ana Paula Furlani, Eduardo Mastalir, Paulo Lavanière Moreno, Sang Won Han, Eduardo Ludwig, Gabriel Grossman, João Ricardo Michielin Sant'Anna, Guaracy Fernandes Teixeira Filho, Melissa Medeiros Markoski, Andrés Delgado Cañedo, Melissa Camassola, Iran Castro, Maria Cláudia Irigoyen, Luiza Macedo Braga and Rogério Sarmento Leite.
REFERENCES
1 . WHO, World Health Organisation, Cardiovascular Diseases . http://www.who.int/cardiovascular_diseases/prevention_control/en, 2006 .
2. Mannheimer C, Camici P, Chester MR, Collins A, DeJongste M, Eliasson T, et al. The problem of chronic refractory angina: report from the ESC Joint Study Group on the Treatment of Refractory Angina. Eur Heart J. 2002;23(5):355-70. [MedLine]
3. Lloyd-Jones DM, Hong Y, Labarthe D, Mozaffarian D, Appel LJ, Van Horn L, et al. American Heart Association Strategic Planning Task Force and Statistics Committee. Defining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association's strategic Impact Goal through 2020 and beyond. Circulation. 2010;121(4):586-613. [MedLine]
4. Gupta R, Tongers J, Losordo W. Human studies of angiogenic gene therapy. Circ Res. 2009;105(8):724-36. [MedLine]
5. Kim MC, Kini A, Sharma SK. Refractory angina pectoris: mechanism and therapeutic options. J Am Coll Cardiol. 2002;39(6):923-34. [MedLine]
6. Huard J, Li Y, Peng H, Fu FH. Gene therapy and tissue engineering for sports medicine. J Gen Med. 2003;5(2):93-108.
7. Karthikeyan BV, Pradeep AR. Gene therapy in periodontics: a review and future implications. J Contemp Dent Pract. 2006;7(3):83-91. [MedLine]
8. Li SD, Huang L. Gene therapy progress and prospects: non-viral gene therapy by systemic delivery. Gene Ther. 2006;13(18):1313-9. [MedLine]
9. Svensson EC, Marshall DJ, Woodard K, Lin H, Jiang F, Chu L. Efficient and stable transduction of cardiomyocytes after intramyocardial injection or intracoronary perfusion with recombinant adeno-associated virus vectors. Circulation. 1999;99(2):201-5. [MedLine]
10. Rafii S, Lyden D. Therapeutic stem and progenitor cell transplantation for organ vascularization and regeneration. Nat Med. 2003;9(6):702-12. [MedLine]
11. Lotufo P. Mortalidade precoce por doenças do coração no Brasil. Comparação com outros países. Arq Bras Cardiol. 1998;70(5):321-5. [MedLine]
12. Kastrup J. Therapeutic angiogenesis in ischemic heart disease: gene or recombinant vascular growth factor protein therapy? Curr Gene Ther. 2003;3(3):197-206. [MedLine]
13. Isner JM. Myocardial gene therapy. Nature. 2002;415(6868):234-9. [MedLine]
14. Rakusan K. Coronary angiogenesis. From morphometry to molecular biology and back. Ann N Y Acad Sci. 1995;752:257-66. [MedLine]
15. Takeshita S, Zheng LP, Brogi E, Kearney M, Pu LQ, Bunting S, et al. Therapeutic angiogenesis. A single intraarterial bolus of vascular endothelial growth factor augments revascularization in a rabbit ischemic hind limb model. J Clin Invest. 1994;93(2):662-70. [MedLine]
16. Kones R. Recent advances in the management of chronic stable angina I: approach to the patient, diagnosis, pathophysiology, risk stratification, and gender disparities. Vasc Health Risk Manag. 2010;6:635-56. [MedLine]
17. Armstrong EJ, Bischoff J. Heart valve development: endothelial cell signaling and differentiation. Circ Res. 2004;95(5):459-70. [MedLine]
18. Habeck M. Wielding more power over angiogenesis. Mol Med Today. 2000;6(4):138-9. [MedLine]
19. Lewis BS, Flugelman MY, Weisz A, Keren-Tal I, Schaper W. Angiogenesis by gene therapy: a new horizon for myocardial revascularization? Cardiovasc Res. 1997;35(3):490-7. [MedLine]
20. Ripa RS, Wang Y, Jørgensen E, Johnsen HE, Hesse B, Kastrup J. Intramyocardial injection of vascular endothelial growth factor-A165 plasmid followed by granulocyte-colony stimulating factor to induce angiogenesis in patients with severe chronic ischaemic heart disease. Eur Heart J. 2006;27(15):1785-92. [MedLine]
21. Kastrup J, Jørgensen E, Rück A, Tägil K, Glogar D, Ruzyllo W, et al; Euroinject One Group. Direct intramyocardial plasmid vascular endothelial growth factor-A165 gene therapy in patients with stable severe angina pectoris A randomized double-blind placebo-controlled study: the Euroinject One trial. J Am Coll Cardiol. 2005;45(7):982-8. [MedLine]
22. Hedman M, Hartikainen J, Syvänne M, Stjernvall J, Hedman A, Kivelä A, et al. Safety and feasibility of catheter-based local intracoronary vascular endothelial growth factor gene transfer in the prevention of postangioplasty and in-stent restenosis and in the treatment of chronic myocardial ischemia: phase II results of the Kuopio Angiogenesis Trial (KAT). Circulation. 2003;107(21):2677-83. [MedLine]
23. Eppler SM, Combs DL, Henry TD, Lopez JJ, Ellis SG, Yi JH, et al. A target-mediated model to describe the pharmacokinetics and hemodynamic effects of recombinant human vascular endothelial growth factor in humans. Clin Pharmacol Ther. 2002;72(1):20-32. [MedLine]
24. Simons M, Annex BH, Laham RJ, Kleiman N, Henry T, Dauerman H, et al. Pharmacological treatment of coronary artery disease with recombinant fibroblast growth factor-2: double-blind, randomized, controlled clinical trial. Circulation. 2002;105(7):788-93. [MedLine]
25. Losordo DW, Vale PR, Hendel RC, Milliken CE, Fortuin FD, Cummings N, et al. Phase 1/2 placebo-controlled, double-blind, dose-escalating trial of myocardial vascular endothelial growth factor 2 gene transfer by catheter delivery in patients with chronic myocardial ischemia. Circulation. 2002;105(17):2012-8. [MedLine]
26. Sylvén C, Sarkar N, Rück A, Drvota V, Hassan SY, Lind B, et al. Myocardial Doppler tissue velocity improves following myocardial gene therapy with VEGF-A165 plasmid in patients with inoperable angina pectoris. Coron Artery Dis. 2001;12(3):239-43. [MedLine]
27. Rosengart TK, Lee LY, Patel SR, Sanborn TA, Parikh M, Bergman GW, et al. Angiogenesis gene therapy: phase I assessment of direct intramyocardial administration of an adenovirus vector expressing VEGF121 cDNA to individuals with clinically significant severe coronary artery disease. Circulation. 1999;100(5):468-74. [MedLine]
28. Hedman M, Hartikainen J, Syvänne M, Stjernvall J, Hedman A, Kivelä A, et al. Safety and feasibility of catheter-based local intracoronary vascular endothelial growth factor gene transfer in the prevention of postangioplasty and in-stent restenosis and in the treatment of chronic myocardial ischemia: phase II results of the Kuopio Angiogenesis Trial (KAT). Circulation. 2003;107(21):2677-83. [MedLine]
29. Kalil R. Terapia gênica aplicada à cirurgia cardiovascular. Rev da SOCERGS. 2001;3:61-6.
30. Kalil R, Sant'Anna R. Terapia gênica aplicada às doenças cardiovasculares. Rev SOCERGS. 2004;3:213-9.
31. Heiss C, Amabile N, Lee AC, Real WM, Schick SF, Lao D, et al. Brief secondhand smoke exposure depresses endothelial progenitor cells activity and endothelial function: sustained vascular injury and blunted nitric oxide production. J Am Coll Cardiol. 2008;51(18):1760-71. [MedLine]
32. Hristov M, Erl W, Weber PC. Endothelial progenitor cells: mobilization, differentiation, and homing. Arterioscler Thromb Vasc Biol. 2003;23(7):1185-9. [MedLine]
33. Hambrecht R, Wolf A, Gielen S, Linke A, Hofer J, Erbs S, et al. Effect of exercise on coronary endothelial function in patients with coronary artery disease. N Engl J Med. 2000;342(7):454-60. [MedLine]
34. Kawasuji M, Nagamine H, Ikeda M, Sakakibara N, Takemura H, Fujii S, et al. Therapeutic angiogenesis with intramyocardial administration of basic fibroblast growth factor. Ann Thorac Surg. 2000;69(4):1155-61. [MedLine]
35. Azuma J, Taniyama Y, Takeya Y, Iekushi K, Aoki M, Dosaka N, et al. Angiogenic and antifibrotic actions of hepatocyte growth factor improve cardiac dysfunction in porcine ischemic cardiomyopathy. Gene Ther. 2006;13(16):1206-13. [MedLine]
36. Morishita R, Aoki M, Hashiya N, Yamasaki K, Kurinami H, Shimizu S, et al. Therapeutic angiogenesis using hepatocyte growth factor (HGF). Curr Gene Ther. 2004;4(2):199-206. [MedLine]
37. Yang ZJ, Xu SL, Chen B, Zhang SL, Zhang YL, Wei W, et al. Hepatocyte growth factor plays a critical role in the regulation of cytokine production and induction of endothelial progenitor cell mobilization: a pilot gene therapy study in patients with coronary heart disease. Clin Exp Pharmacol Physiol. 2009;36(8):790-6. [MedLine]
38. Bae J, Cho M. Gene therapy for heart failure. Korean Circ J. 2005;35(5):345-52.
39. Giordano FJ, Ping P, McKirnan MD, Nozaki S, DeMaria AN, Dillmann WH, et al. Intracoronary gene transfer of fibroblast growth factor-5 increases blood flow and contractile function in an ischemic region of the heart. Nat Med. 1996;2(5):534-9. [MedLine]
40. Wright MJ, Wightman LM, Lilley C, de Alwis M, Hart SL, Miller A, et al. In vivo myocardial gene transfer: optimization, evaluation and direct comparison of gene transfer vectors. Basic Res Cardiol. 2001;96(3):227-36. [MedLine]
41. Wilson DR. Viral-mediated gene transfer for cancer treatment. Curr Pharm Biotechnol. 2002;3(2):151-64. [MedLine]
42. Rubanyi GM. The future of human gene therapy. Molecular Aspects Med. 2001;22(3):113-42.
43. Dulak J, Zagorska A, Wegiel B, Loboda A, Jozkowicz A. New strategies for cardiovascular gene therapy: regulatable pre-emptive expression of pro-angiogenic and antioxidant genes. Cell Biochem Biophys. 2006;44(1):31-42. [MedLine]
44. Mack CA, Patel SR, Schwarz EA, Zanzonico P, Hahn RT, Ilercil A, et al. Biologic bypass with the use of adenovirus-mediated gene transfer of the complementary deoxyribonucleic acid for vascular endothelial growth factor 121 improves myocardial perfusion and function in the ischemic porcine heart. J Thorac Cardiovasc Surg. 1998;115(1):168-76.
45. Losordo DW, Vale PR, Symes JF, Dunnington CH, Esakof DD, Maysky M, et al. Gene therapy for myocardial angiogenesis: initial clinical results with direct myocardial injection of phVEGF165 as sole therapy for myocardial ischemia. Circulation. 1998;98(25):2800-4. [MedLine]
46. Henry TD, Annex BH, McKendall GR, Azrin MA, Lopez JJ, Giordano FJ, et al; VIVA Investigators. The VIVA trial: Vascular endothelial growth factor in Ischemia for Vascular Angiogenesis. Circulation. 2003;107(10):1359-65. [MedLine]
47. Hendel RC, Henry TD, Rocha-Singh K, Isner JM, Kereiakes DJ, Giordano FJ, et al. Effect of intracoronary recombinant human vascular endothelial growth factor on myocardial perfusion: evidence for a dose-dependent effect. Circulation. 2000;101(2):118-21. [MedLine]
48. Symes JF, Losordo DW, Vale PR, Lathi KG, Esakof DD, Mayskiy M, et al. Gene therapy with vascular endothelial growth factor for inoperable coronary artery disease. Ann Thorac Surg. 1999;68(3):830-6.
49. Vale PR, Losordo DW, Milliken CE, Maysky M, Esakof DD, Symes JF, et al. Left ventricular electromechanical mapping to assess efficacy of phVEGF(165) gene transfer for therapeutic angiogenesis in chronic myocardial ischemia. Circulation. 2000;102(9):965-74. [MedLine]
50. Reilly JP, Grise MA, Fortuin FD, Vale PR, Schaer GL, Lopez J, et al. Long-term (2-year) clinical events following transthoracic intramyocardial gene transfer of VEGF-2 in no-option patients. J Interv Cardiol. 2005;18(1):27-31. [MedLine]
51. Stewart DJ, Hilton JD, Arnold JM, Gregoire J, Rivard A, Archer SL, et al. Angiogenic gene therapy in patients with nonrevascularizable ischemic heart disease: a phase 2 randomized, controlled trial of AdVEGF(121) (AdVEGF121) versus maximum medical treatment. Gene Ther. 2006;13(21):1503-11. [MedLine]
52. Ruel M, Beanlands RS, Lortie M, Chan V, Camack N, deKemp RA, et al. Concomitant treatment with oral L-arginine improves the efficacy of surgical angiogenesis in patients with severe diffuse coronary artery disease: the Endothelial Modulation in Angiogenic Therapy randomized controlled trial. J Thorac Cardiovasc Surg. 2008;135(4):762-70.
53. Kalil RAK, Salles FB, Giusti II, Rodrigues CG, Han SW, Sant'anna RT, et al. Terapia gênica com VEGF para angiogênese na angina refratária: ensaio clínico fase I/II. Rev Bras Cir Cardiovasc. 2010;25(3):311-21. [MedLine] View article
54. Vale PR, Losordo DW, Milliken CE, McDonald MC, Gravelin LM, Curry CM, et al. Randomized, single-blind, placebo-controlled pilot study of catheter-based myocardial gene transfer for therapeutic angiogenesis using left ventricular electromechanical mapping in patients with chronic myocardial ischemia. Circulation. 2001;103(17):2138-43. [MedLine]
55. Kastrup J, Jørgensen E, Rück A, Tägil K, Glogar D, Ruzyllo W, et al; Euroinject One Group. Direct intramyocardial plasmid vascular endothelial growth factor-A165 gene therapy in patients with stable severe angina pectoris A randomized double-blind placebo-controlled study: the Euroinject One trial. J Am Coll Cardiol. 2005;45(7):982-8. [MedLine]
56. Ripa RS, Wang Y, Jørgensen E, Johnsen HE, Hesse B, Kastrup J. Intramyocardial injection of vascular endothelial growth factor-A165 plasmid followed by granulocyte-colony stimulating factor to induce angiogenesis in patients with severe chronic ischaemic heart disease. Eur Heart J. 2006;27(15):1785-92. [MedLine]
57. Stewart DJ, Kutryk MJ, Fitchett D, Freeman M, Camack N, Su Y, et al. VEGF gene therapy fails to improve perfusion of ischemic myocardium in patients with advanced coronary disease: results of the NORTHERN trial. Mol Ther. 2009;17(6):1109-15. [MedLine]
58. Grines CL, Watkins MW, Helmer G, Penny W, Brinker J, Marmur JD, et al. Angiogenic Gene Therapy (AGENT) trial in patients with stable angina pectoris. Circulation. 2002;105(11):1291-7. [MedLine]
59. Grines CL, Watkins MW, Mahmarian JJ, Iskandrian AE, Rade JJ, Marrott P, et al; Angiogene GENe Therapy (AGENT-2) Study Group. A randomized, double-blind, placebo-controlled trial of Ad5FGF-4 gene therapy and its effect on myocardial perfusion in patients with stable angina. J Am Coll Cardiol. 2003;42(8):1339-47. [MedLine]
60. Henry TD, Grines CL, Watkins MW, Dib N, Barbeau G, Moreadith R, et al. Effects of Ad5FGF-4 in patients with angina: an analysis of pooled data from the AGENT-3 and AGENT-4 trials. J Am Coll Cardiol. 2007;50(11):1038-46. [MedLine]
61. Powell RJ, Simons M, Mendelsohn FO, Daniel G, Henry TD, Koga M, et al. Results of a double-blind, placebo-controlled study to assess the safety of intramuscular injection of hepatocyte growth factor plasmid to improve limb perfusion in patients with critical limb ischemia. Circulation. 2008;118(1):58-65. [MedLine]
62. Hamawy AH, Lee LY, Crystal RG, Rosengart TK. Cardiac angiogenesis and gene therapy: a strategy for myocardial revascularization. Curr Opin Cardiol. 1999;14(6):515-22. [MedLine]
63. Hao X, Månsson-Broberg A, Grinnemo KH, Siddiqui AJ, Dellgren G, Brodin LA, et al. Myocardial angiogenesis after plasmid or adenoviral VEGF-A(165) gene transfer in rat myocardial infarction model. Cardiovasc Res. 2007;73(3):481-7. [MedLine]
64. Rana JS, Mannam A, Donnell-Fink L, Gervino EV, Sellke FW, Laham RJ. Longevity of the placebo effect in the therapeutic angiogenesis and laser myocardial revascularization trials in patients with coronary heart disease. Am J Cardiol. 2005;95(12):1456-9 [MedLine]
65. Kalil RA, Teixeira LA, Mastalir ET, Moreno P, Fricke CH, Nardi NB. Experimental model of gene transfection in healthy canine myocardium: perspectives of gene therapy for ischemic heart disease. Arq Bras Cardiol. 2002;79(3):223-32. [MedLine]
66. Sant'Anna RT, Kalil RAK, Moreno P, Anflor LCJ, Correa DLC, Ludwig R, et al. Gene therapy with VEGF 165 for angiogenesis in experimental acute myocardial infarction. Rev Bras Cir Cardiovasc. 2003;18(2):142-7. View article
67. Furlani A, Kalil RA, Castro I, Cañedo-Delgado A, Barra M, Prates PR, et al. Effects of therapeutic angiogenesis with plasmid VEGF165 on ventricular function in a canine model of chronic myocardial infarction. Rev Bras Cir Cardiovasc. 2009;24(2):143-9. [MedLine] View article
68. Murasawa S, Asahara T. Endothelial progenitor cells for vasculogenesis. Physiology (Bethesda). 2005;20:36-42. [MedLine]
Article receive on Tuesday, June 14, 2011
 All scientific articles published at rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at rbccv.org.br are licensed under a Creative Commons license



All rights reserved 2017 / © 2025 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()
 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}