![]()
![]()
Jarbas Jakson DinkhuysenI; Aron Jose Pazin de AndradeII; Juliana LemeIII; Cibele SilvaIV; Claudia Sanches MedinaIII; Cristiane Célia PereiraIII; José Francisco BiscegliII
DOI: 10.5935/1678-9741.20140095
RESUMO
OBJETIVOS: Apresentar resultados da aplicação da bomba espiral que emprega efeitos hidráulicos centrífugo e axial de bombeamento como elemento propulsor do circuito de circulação extracorpórea em pacientes submetidos a cirurgias cardíacas após modificações introduzidas no design do projeto original.
MÉTODOS: O estudo foi realizado em 52 pacientes (51% masculinos), com idade entre 20 a 80 (67±14,4) anos, peso 53 a 102 (71,7±12,6) kg, submetidos na maioria a cirurgia de revascularização miocárdica (34,6%) e Orovalvar (32,8%). Além das avaliações rotineiras, foram registrados rotação, tempo de CEC e para análise do impacto traumático à crase sanguínea, hemoglobina livre na urina (+ a 4+), desidrogenase láctica, fibrinogênio (mg/dL) e contagem de plaquetas (nº/mm3).
RESULTADOS: Observou-se a manutenção de parâmetros pressóricos e metabólicos adequados. Quanto aos marcadores de danos à crase sanguínea, as alterações estiveram proporcionais ao tempo maior de circulação extracorpórea. Os níveis de Hemoglobina Livre permaneceram com valores normais, com ligeiro aumento a partir dos 90 minutos de circulação extracorpórea. A Desidrogenase Láctica mostrou aumento, variando as medianas entre 550 a 770 UI/L enquanto o Fibrinogênio mostrou queda das medianas de 130 a 100 mg/dl. O número de plaquetas mostrou ligeira queda das medianas variando entre 240.000 a 200.000/mm3. Não ocorreram dificuldades de saída de perfusão, não se observou óbito imediato e todos os pacientes, exceto 1, obtiveram alta hospitalar.
CONCLUSÃO: A bomba espiral aplicada como bomba propulsora de sangue durante cirurgia cardíaca se mostrou confiável e segura, não causou impacto traumático à crase sanguínea importante e se constitui opção como dispositivo original, concebido em nosso meio.
ABSTRACT
OBJECTIVE: The objective of this paper is to present the results from Spiral Pump clinical trial after design modifications performed at its previous project. This pump applies axial end centrifugal hydraulic effects for blood pumping during cardiopulmonary bypass for patients under cardiac surgery.
METHODS: This study was performed in 52 patients (51% males), between 20 to 80 (67±14.4) years old weighing 53 to 102 (71.7±12.6) kg, mostly under myocardial revascularization surgery (34.6%) and valvular surgery (32.8%). Besides the routine evaluation of the data observed in these cases, we monitored pump rotational speed, blood flow, cardiopulmonary bypass duration, urine free hemoglobin for blood cell trauma analysis (+ to 4+), lactate desidrogenase (UI/L), fibrinogen level (mg/dL) and platelet count (nº/mm3).
RESULTS: Besides maintaining appropriate blood pressure and metabolic parameters it was also observed that the Free Hemoglobin levels remained normal, with a slight increase after 90 minutes of cardiopulmonary bypass. The Lactate Dehydrogenase showed an increase, with medians varying between 550-770 IU/L, whereas the decrease in Fibrinogen showed medians of 130-100 mg/dl. The number of platelets showed a slight decrease with the medians ranging from 240,000 to 200,000/mm3. No difficulty was observed during perfusion terminations, nor were there any immediate deaths, and all patients except one, were discharged in good condition.
CONCLUSION: The Spiral Pump, as blood propeller during cardiopulmonary bypass, demonstrated to be reliable and safe, comprising in a good option as original and national product for this kind of application.
ACT: Activated Coagulation Time
SMR: Surgical Myocardial Revascularization
CPB: cardiopulmonary bypass
ETO: Ethylene oxide
IDPC: Institute Dante Pazzanese of Cardiology
LD: Lactate Dehydrogenase
MAP: Medial arterial pressure
SP: Spiral Pump
INTRODUCTION
The Division of Bioengineering from Instituto Dante Pazzanese de Cardiologia (IDPC) started in 1992 a research aiming to develop a blood pump for cardiopulmonary bypass (CPB), called Spiral Pump® (SP). The SP was idealized as a device to drive blood minimizing damage to blood cells during CPB[1-3], and also, providing lower cost by being produced in Brazil protected by a Patent of Invention number PI 91,022,215 from the National Institute of Industrial Property.
SP uses two hydraulic pumping principles simultaneously, centrifugal and axial, provided by conically shaped rotor with threads on its surface, increasing the hydrodynamic pumping performance without increasing rates of blood cell damage such as hemolysis[4].
Between 1994 and 1999, a pilot number of devices was produced, for in vivo tests (sheep), based on an experimental protocol, approved by IDPC's Experimental Research Ethics Committee. SP was used as a pumping device for CPB. From 1999 to 2002, clinical evaluations were performed on 43 patients during cardiac surgery with CPB[5]. After approved in clinical evaluations, the device was registered at the National Health Surveillance Agency (ANVISA) under number 10264470020.
In 2007, the development of a new rotor design had started, using two entrances at the threads of the spiral impeller pumps and also, modifying the device external base, aiming to have same coupling system as other devices, allowing its use routinely in cardiac surgeries. During this improvement process, many additional in vitro and in vivo tests were performed[5-9].
A new in vivo tests were performed according to a new experiment protocol, number 2010/003, approved by the IDPC's Ethics Committee for Animal Usage, and with those new results, SP was able to undergo to a new clinic evaluation phase. For this phase, new devices were assembled inside controlled environment, according to ISO 14644, ISO 8 and ISO 13485, and sterilized by ethylene oxide (ETO)[9].
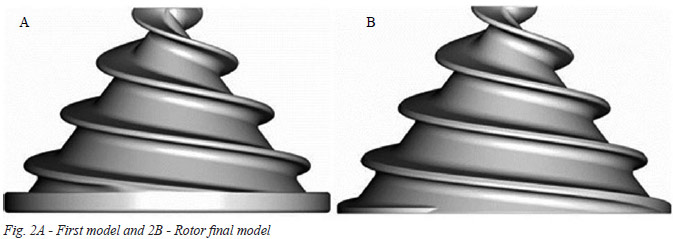
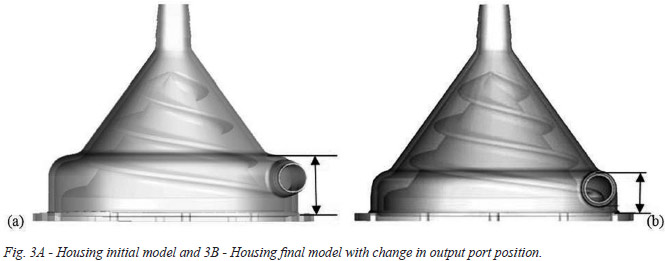
As the original prototype (Figure 1A), this new model uses centrifugal and axial forces simultaneously as hydraulic principles, improving its hydrodynamic performance without increasing blood damage. This pump has in its interior a spiral conic rotor to generate pumping pressures. Axial pumping effect is produced due to double entrance threads at impeller surface, and centrifugal pumping effect occurs because of impeller conical shape. At the top of the housing, there is the inlet port and, at the bottom, the outlet port, both with 3/8-inch connections (Figure 1B). Housing base consists of a plastic disc with one stainless steel shaft that holds all internal pump components. Housing base provides total isolation between pump inside and outside. Motor torque is transmitted to spiral impeller by magnetic coupling, using two annular magnets, one inside the impeller and another fixed to the shaft of the driver motor.
Preliminary studies have shown that changes in rotor design caused important changes in device performance and positive impact was noted during hemolysis tests due to the new conical shape and new rotor design, as well as making lower the pump outlet port (Figures 2 and 3)[6,7]. Previous studies, conducted in 1998, showed that the original pump performance was 3000 rpm under a pressure of 350 mmHg, and under similar pumping flow as the reference model Biopump® (BPX80, Medtronic, USA). However, it was around 2500 rpm for the same pressure with the new SP model[5,7].
Objectives
This work aims to conduct clinical evaluation with Spiral Pump (SP) during cardiopulmonary bypass (CPB), as an impeller blood pump for patients under cardiac surgery.
METHODS
Inclusion criteria:
• Indication for cardiac surgery with CPB in most myocardial revascularization and orovalvular lesions;
• With or without cardioplegia;
• Age between 40 and 80 years;
• Male and female;
• Body weight between 55 and 120 kg.
Exclusion criteria:
• Cardiac surgery without CPB;
• Abnormalities in laboratory tests (coagulogram);
• Surgery for patients with underweight (<55 kg).
Study was conducted in a group of 52 patients, 27 male (52%), age of 20-80 (67.0±14.4) years, weight of 53-102 (71.7±12.6) kg.
Indications for surgery were:
• Surgical Myocardial Revascularization (SMR) 19 (36.5%);
• Orovalvar surgery 17 (32.6%), SMR + orovalvar 11 (21.1%);
• Other 2 (3.8%);
• Valvar + other 1 (1.9%);
• Congenital + orovalvar 1 (1.9%);
• Congenital 1 (1.9%).
CPB circuit components were: SP, drive module (Bioconsole 550®, Medtronic, Minneapolis, USA), flowmeter (Bioprobe® TX50, Medtronic, Minneapolis, USA), CPB machine (Macchi, Sao Paulo, Brazil), tube kit with blood filter (Nipro Medical, Sorocaba, Brazil), Vital adult membrane oxygenator (Nipro Medical, Sorocaba, Brazil) (in 18 cases) and Quadrox adult oxygenator - Softlibe Coating and adult hemoconcentrator - HPH 1000 (Maquet, Germany) (in 34 cases).
All clinical evaluation procedures were performed by the same surgeon, principal investigator, and two perfusionists to maintain reliable results.
Routine procedures for cardiac surgeries were used, such as general anesthesia with endotracheal intubation for pulmonary ventilation, assessment of body temperature by an esophageal thermometer, assessment of average medial arterial pressure (MAP) by catheterization of peripheral arterial line and central venous pressure (CVP) by catheterization of central vein, urinary catheterization to evaluate urinary flow and heart rate monitoring with specific monitor.
The exposure of the heart was performed by median thoracotomy and, after systemic heparinization (5 mg/kg), CPB was installed by the ascending aorta or femoral artery for oxygenated blood intake from the oxygenator, pumped by the SP, and, from the right atrium, with single cannula or selective of higher and lower cava to drain venous blood toward the membrane oxygenator reservoir to CO2/O2 exchange.
After CPB initiation and stabilization of metabolic and perfusion parameters with esophageal temperature around 32ºC, pulmonary ventilation was stopped and the perfusionist, every 5 minutes, took balance notes from MAP, CVP, diuresis, temperature, flow and occasional events. As usual, at the beginning, middle and end of the procedure, samples for laboratory tests were collected (blood gases, A/V, K+, Na+, hematocrit, glucose) that were used as standard for possible therapeutic interventions during the procedure. The anticoagulation control during CPB were performed by measuring Activated Coagulation Time (ACT) in an activated coagulation monitor MCA2000 (Adib Jatene Foundation, Sao Paulo, Brazil), trying to keep it above 500 seconds. At the end of CPB, reversion of heparin was performed with protamine sulfate, as previously established standard. Completing the surgical procedure, the patient was taken to Postoperative Recovery Unit under mechanical ventilation, ECG monitoring and MAP, diuresis and temperature controls.
In order to evaluate the interactions between SP and blood, specific investigated parameters in this study were: LDH (U/L), fibrinogen (g/L), platelet count (no/mm3), ACT (seconds) and the urinalysis tape in pre CPB (5 minutes before), every 15 minutes during the procedure and after CPB (5 minutes after infusion) in all patients in the operating room before being referred to the Postoperative Recovery Unit.
For subsequent evaluation, ACT was determined for the period that preceded the CPB, during (30, 60, 90 and 120 minutes) and after anticoagulation reversing at the end of the procedure.
All patients have been previously contacted by researchers in the preoperative period, according to surgery schedule, and were told about the study objectives, risks and benefits, in accordance to Informed Consent Statement signed by each participant of the Clinical Evaluation Protocol, No. 4072 of April 5, 2011, approved by IDPC´s Research Ethics Committee.
Statistical analysis
Describing patient samples, attendance and percentage were used for qualitative variables and average, standard deviation, median and interquartile range for quantitative variables.
Two-tailed Fisher's exact tests were made for qualitative variables and Kruskal Wallis for quantitative ones. For the variables that have association (P<0,05) in the Kruskal Wallis tests, multiple comparisons were made (2 by 2 tests), through the non parametric Turkey method, to verify which groups are different between themselves.
ANOVA non-parametric tests were also performed, with time being the only factor, with n greater than or equal to 5. Charts profiles were used with 95% confidence intervals for the averages.
RESULTS
Time of CPB ranged from 30 to 240 (111.2±47.7) minutes in all cases and no problem was observed during perfusion outcome.
There are 12 graphs in Figure 4 with observed parameters from device clinical evaluation. First graph shows rotational speed of SP during CPB, always related to weight (body surface area) for each patient, small variations between 2000 - 2500 rpm were observed. The flow provided by SP (second graph) shows oscillations from 3.7 to 3.3 L/min with a higher standard deviation at final moments during the procedure.
Considering as appropriate the MAP value of 60 mmHg during CPB, we observed that the curve oscillates right below this level with higher standard deviation at final moments during the procedure (third graph), this fact has not caused any organic damage due to the lowering of esophageal temperature near 30ºC, reducing the metabolic and perfusion requirements. Urinary volume generated during CPB varied around 150 ml at first moments, decreasing around 100 ml from 30 to 150 minutes (fourth graph). Related to laboratory data, we emphasize that all time scales of the following graphs ranged from pre CPB, 0-120 minutes and post CPB.
The pH values ranged close to normal values of 7.45 (fifth graph), with larger oscillation after 75 minutes until the end of the procedure. The Sodium (Na) levels (sixth graph) ranged below 139 mg/L and increased after 90 minutes of perfusion, maintaining this level until the end of the procedure, so did the Potassium (K) levels (seventh graph). As expected, the hematocrit (Ht) showed significant decrease after perfusion initiation, this is due to hemodilution imposed by oxygenator priming, usually with saline solutions, and remained around 30% until 105 minutes, increasing at the end of the procedure (eighth graph), the same occurs to hemoglobin (Hb) values (ninth graph). Blood glucose (tenth graph) varied around 130 mg/L initially to levels near 200 mg/L at final moments of CPB and considering infusion of serum glycosylated during anesthesia.
ACT analysis (eleventh graph) shows adequate levels of anticoagulation during procedure, ranging from 1500 to 1800 seconds. Finally, free hemoglobin analysis from urine, which represents the mechanical trauma impact to the blood (twelfth graph), shows levels close to 0 within 90 minutes, when we observed an increase of values from 0 to 1 with increased standard deviation, common fact observed at the end of CPB.
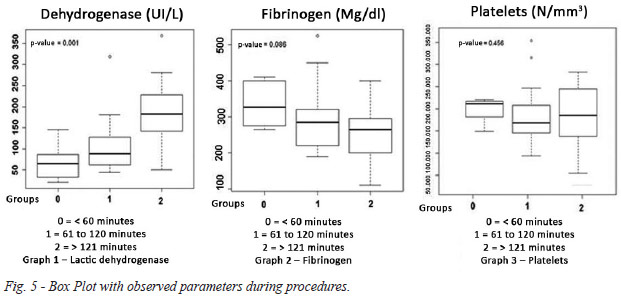
Considering the values of lactic dehydrogenase, we observed an increase of the medians ranging between 500-770 IU/L (Figure 5 and Chart 1). The levels of fibrinogen showed a decrease of medians between 130-100 mg/dl (Figure 5 and Chart 2), both proportional to higher CPB time. Related to number of platelets (Figure 5 and Chart 3), the medians ranged between 240,000/m3 for the 0 to 60 minutes of CPB group and 20,000/mm3 for the 0 to >120 minutes group, denoting small traumatic impact to the blood.
The values of lactic dehydrogenase (VN 305UI/L) in pre CPB ranged between 238-994 (427.6±134.5) and post CPB between 380-1954 (926.7±350.1) IU/L. Fibrinogen values (VN 200-400 mg/dl) before CPB ranged between 164.2 to 403.2 (267±56.4) and after CPB between 145.5 to 439.3 (215.3±48.1) mg/dl, and Platelet (VN 150000-400000/mm3) showed before CPB between 103000-307000 (209.100±64.900/mm3) and after CPB between 66000-233000 (146,000 ± 43,000/m3).
Figure 5 shows the Box Plot analyzing the percentage of Lactate Dehydrogenase (Chart 1), fibrinogen (Chart 2) and Platelet Count (Chart 3) for three groups of patients, a CPB group from 0 to 60 minutes, a group from 0 to 120 minutes and a group with time above 120 minutes, observing the expected results for this procedure.
There were no immediate deaths, observing ICU stay ranged from 1 to 4 (average 2.4) days. One patient remained 13 and another remained 44 days for presenting postoperative complications that required intensive controls, the patients in question were diabetic and smokers, complicating the postoperative period. One death occurred on the 1st postoperative day due to bleeding by clotting disorder.
Patients were discharged from 3 to 14 (average 6.5) days and only one remained for longer due to postoperative complications and for being diabetic and smoker, and was discharged on the 61st postoperative day in good condition.
DISCUSSION
During the project development, the rapid prototyping process helped to make possible the construction and assembly of different SP models in a short period of time, moreover, allowed cost reduction in the manufacture of disposable product process, to avoid costly manufacturing of different plastic injection molds.
Various changes were performed to hydrodynamically test the performance curves (pressure x flow), showing that, for each prototype, changes in pumping characteristics were made, until we reach the most efficient one, that has been selected for clinical use[4,5].
While developing the design of medical products, such as blood pumps for CPB, patients can be adversely affected by the use of devices that may cause high levels of plasma free hemoglobin, especially in the postoperative period. Therefore, the project is based on consistent in vitro and in vivo tests that can generate product with good acceptance and competitiveness for clinical application[6].
Structural characteristics of a blood pump are important in determining its hydrodynamic performance and blood trauma. Often, small structural changes cause large changes to the results, as shown in this work[6].
Currently, roller pumps are used in cardiac surgery and centrifugal pumps for severe cases. The roller pump is widely used due to low cost, easy usage and simplicity, its flow is linear with slight pulsatility, but generates high negative pressure when sucking blood to the CPB circuit, which can cause major blood damages[10]. Centrifugal pumps, mostly imported, have higher costs, so they are not often used. The development of a blood pump with national technology and low cost will enable more often usage in public and private hospitals.
During CPB, the flow, provided by a centrifugal pump, depends on the motor rotational speed and on the pump output pressure that depends on the pressure drop of CPB circuit and on its after load. Thus, when the peripheral resistance of the patient increases, the blood pressure will increase also, causing decrease in the pump flow. This is a self-compensatory effect that does not happen in peristaltic roller pumps. Roller pumps provide a constant flow for a fixed rotation of the motor, in other words, independent of blood pressure. So, if an increase in peripheral resistance of the patient occurs, the blood pressure will rise too much, causing risks to the patient[11].
Compression of blood between collapsed structures, heating, friction during pumping, irregular surfaces, turbulent flows, the stagnation flow and the rapid pressure variations are among the main mechanisms of trauma in these devices.
Hemolysis is always a reason for conducting research for development of blood pumps, it is impossible to avoid it completely, so maintaining close to normal values found in the literature is necessary[11].
Group under study consisted of adult patients undergoing cardiac surgery with conventional CPB and SP as blood pump. In the procedures, perfusions during heart surgery were followed from pre CPB to post CPB and, in this period, the operating data of SP, such as rotational speed, blood flow, vibration and noise were controlled and were considered satisfactory according to standards for cardiac surgery. The flow data, comparing to the theoretical flow calculated for each patient, were within our expectations and attending the needs for perfusion during surgery, demonstrating that SP is suitable for perfusion of adult patients.
Physiological and laboratory parameters such as diuresis, mean arterial pressure, temperature and blood gas data were recorded. The selected as hemolysis indicators were hemoglobin and hematocrit, which were satisfactory by means of comparison with normal and expected post-perfusion values found in the literature[11].
In the case of hemoglobin, analysis over time shows that this parameter tends to fall after the first fifteen minutes of perfusion, stabilizing below the reference value and returning to normal after the end of perfusion. The same occurs with the hematocrit, which, before CPB, presents mean values very close to normal minimum value, but still shows higher than expected during perfusion and after CPB.
In most cases, there was no free hemoglobin (Hb) in urine and its presence in urine was seen only in cases over 115 minutes of perfusion. Specific parameters to this study, Lactate Dehydrogenase, Platelets and Fibrinogen, have its analysis performed according to pefusion time. We noted that time has a direct influence on the increase of LDH and decreased platelets and fibrinogen, these parameters are indicators of hemolysis. But the values found are still acceptable for the post CPB, which means that the pumping system was adequate without traumatic impact.
It is important to say that hemolysis mechanically caused is not only a consequence from SP usage, but is a result of a whole perfusion system that includes the pump, arterial filter, oxygenator, hemoconcentrator and plastic tubes.
Cardiac surgery techniques and perfusion time were varied and the SP performance showed suitable for all cases relating to easy rotation/flow adjustment by the perfusionist and noise or vibration absence.
The results from this study demonstrate that the perfusion system with the usage of SP showed changes for indicative parameters within acceptable values and satisfactorily under the requirements for its application in cardiac surgery, being able to be applied safely.
REFERÊNCIAS
1. Pego PMF, Miura F, Higa SS, Moreira LFP, Dallan LA, Chamone DAF, et al. Hemólise em circulação extracorpórea, estudo comparativo entre bomba de rolete e bomba centrífuga. Rev Bras Cir Cardiovasc. 1989;4(3):220-4.
2. Tamari Y, Lee-Sensiba K, Leonard EF, Parnel V, Tortolani AJ. The effects of pressure and flow on hemolysis caused by BIO-Medicus centrifugal pumps and roller pumps. J Thorac Cardiovasc Surg. 1993; 106(6):997-1007. [MedLine]
3. Andrade AJP, Biscegli J, Dinkhuysen J, Sousa JE, Ohashi Y, Hemmings S, et al. Characteristics of Blood Pump Combining the Centrifugal and Axial Pumping Principles. Artif Organs. 1996;20(6):605-12. [MedLine]
4. Dinkhuysen JJ. Bomba Sanguínea Espiral: concepção, desenvolvimento e aplicação clínica de projeto original [Tese de Livre Docência]. São Paulo: Faculdade de Medicina da Universidade de São Paulo, 2005. 115p.
5. Dinkhuysen JJ, Andrade A, Manrique R, Saito CSM, Leme J, Biscegli JF. Bomba Sanguínea Espiral: concepção, desenvolvimento e aplicação clínica do projeto original. Rev Bras Cir Cardiovasc. 2007;22(2):224-34. [MedLine]
6. Leme J. Projeto, Desenvolvimento e Ensaios In Vitro de Novo Modelo de Bomba de Sangue para Circulação Extracorpórea - Bomba Espiral [Dissertação de Mestrado]. Campinas: Faculdade de Engenharia Mecânica, Universidade Estadual de Campinas, 2010. 93p.
7. Leme J, Fonseca J, Bock E, Silva C, Silva BU, Santos AE, et al. A New Model of Centifugal Blood Pump for Cardiopulmonary Bypass: Design Improvement, Performance, and Hemolysis Tests. Artif Organs. 2011;35(5):443-7. [MedLine]
8. Silva C. Ensaios "In Vivo" e Avaliação clínica de Bomba de sangue para circulação Extracorpórea durante cirurgia cardíaca: SPIRAL PUMP [Dissertação de mestrado]. Campinas: Faculdade de Engenharia Mecânica, Universidade Estadual de Campinas, 2013. 96p.
9. Silva C, Silva BV, Leme J, Vebelhart B, Dinkhuysen J, Biscegli JF, et al. "In vivo" evaluation of Centrifugal blood pump for Cardiopulmonary bypass - Spiral Pump. Artif Organs. 2013,37(11):954-7. [MedLine]
10. Vieira Junior FU, Vieira RW, Antunes N, Petrucci O, Oliveira PP, Serra MMP, et al. Análise do perfil hidrodinâmico em diferentes modelos de bombas de roletes utilizadas em CEC. Rev Bras Cir Cardiovasc. 2009;24(2):188-93. [MedLine]
11. Nose Y. Design and development strategy for the Rotary Blood Pump. Artif Organs. 1998;22(6):438-46. [MedLine]
No financial support.
Authors' roles & responsibilities
JJD: Author
AJPA: Coauthor
JL: Coauthor
CS: Coauthor
CSM: Coauthor
CCP: Coauthor
JFB: Coauthor
Article receive on quarta-feira, 2 de outubro de 2013
 All scientific articles published at rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at rbccv.org.br are licensed under a Creative Commons license



All rights reserved 2017 / © 2025 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()


 Read in English
Read in English
 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket









