![]()
![]()
Luiz Fernando KubruslyI; Marina Simões FormighieriII,III; José Vitor Martins LagoII,III; Yorgos Luiz Santos De Salles GraçaIV,V; Ana Cristina Lira SobralIV; Marianna Martins LagoV
DOI: 10.5935/1678-9741.20140125
ABSTRACT
OBJECTIVE: To evaluate the behavior of castor oil-derived polyurethane as a hemostatic agent and tissue response after abdominal aortic injury and to compare it with 2-octyl-cyanoacrylate.
METHODS: Twenty-four Guinea Pigs were randomly divided into three groups of eight animals (I, II, and III). The infrarenal abdominal aorta was dissected, clamped proximally and distally to the vascular puncture site. In group I (control), hemostasis was achieved with digital pressure; in group II (polyurethane) castor oil-derived polyurethane was applied, and in group III (cyanoacrylate), 2-octyl-cyanoacrylate was used. Group II was subdivided into IIA and IIB according to the time of preparation of the hemostatic agent.
RESULTS: Mean blood loss in groups IIA, IIB and III was 0.002 grams (g), 0.008 g, and 0.170 g, with standard deviation of 0.005 g, 0.005 g, and 0.424 g, respectively (P=0.069). The drying time for cyanoacrylate averaged 81.5 seconds (s) (standard deviation: 51.5 seconds) and 126.1 s (standard deviation: 23.0 s) for polyurethane B (P=0.046). However, there was a trend (P=0.069) for cyanoacrylate to dry more slowly than polyurethane A (mean: 40.5 s; SD: 8.6 s). Furthermore, polyurethane A had a shorter drying time than polyurethane B (P=0.003), mean IIA of 40.5 s (standard deviation: 8.6 s). In group III, 100% of the animals had mild/severe fibrosis, while in group II only 12.5% showed this degree of fibrosis (P=0.001).
CONCLUSION: Polyurethane derived from castor oil showed similar hemostatic behavior to octyl-2-cyanoacrylate. There was less perivascular tissue response with polyurethane when compared with cyanoacrylate.
RESUMO
OBJETIVO: Avaliar o comportamento hemostático e a reação tecidual do poliuretano, derivado da mamona, após injúria da aorta abdominal de cobaias e compará-lo com o 2-octil-cianoacrilato.
MÉTODOS: Vinte e quatro cobaias foram divididas aleatoriamente em três grupos de oito animais (I, II e III). A aorta abdominal infrarrenal foi dissecada, pinçada proximal e distalmente ao local que se procedeu à punção vascular. No grupo I (controle), a hemostasia foi feita com digitopressão; no grupo II (poliuretano), aplicou-se o selante vegetal e, no grupo III (cianoacrilato), aplicou-se o 2-octil-cianoacrilato. O grupo II foi subdividido em IIA e IIB, conforme o tempo de preparo do poliuretano.
RESULTADOS: A média de perda sanguínea nos grupos IIA, IIB e III foi 0,002 g, 0,008 g e 0,170 g, com desvios padrões de 0,005 g, 0,005 g e 0,424 g, respectivamente (P=0,069). O tempo de secagem do selante cianoacrilato foi em média 81,5 segundos (s) (desvio padrão: 51,5 s), enquanto o poliuretano B levou 126,1 segundos (desvio padrão: 23,0 s) (P=0,046). Entretanto, houve tendência (P=0,069) do cianoacrilato apresentar um tempo maior de secagem que o poliuretano A. Além disso, o poliuretano A teve um tempo de secagem menor que o poliuretano B (P=0,003), com média para o IIA de 40,5 segundos (desvio padrão: 8,6 s). No grupo III, 100% dos animais tiveram fibrose moderada/acentuada, enquanto no grupo II apenas 12,5% (P=0,001).
CONCLUSÃO: O poliuretano derivado da mamona apresentou comportamento hemostático semelhante ao 2-octil-cianoacrilato. A cola vegetal demonstrou menor reação tecidual perivascular.
INTRODUCTION
Hemostatic control of small vessels sutures is a crucial point in cardiovascular surgeries and demands great experience of the surgeon[1]. Nevertheless, bleeding through the suture line is a major cause of mortality. In other areas such as surgical trauma, solid organs such as liver and spleen may also have bleeding or may difficult to control due to friability and high vascularization[2].
One major concern is the length of clamping time during vascular injury repair, considering the ischemic damage observed in terminal organs-the longer the ischemia, the more severe the organ injury. Therefore, it is crucial to minimize the duration of ischemia in any type of vascular injury[3].
In the search for a simpler and faster technique, alternative methods of anastomosis have been studied, such as the use of mechanical connecting devices. However, those devices are impractical in some contexts, for instance, when there is a discrepancy in the caliber of the vessels to be joined by anastomosis. Another alternative are vascular sealants such as cyanoacrylate and fibrin glue, a synthetic and a natural (biological) adhesive, respectively[1].
The mechanism of action of cyanoacrylate is polymerization on contact with proteins that function as catalysts, leaving a crust on the lesion surface. Among the cyanoacrylate characteristics worth emphasizing are its bactericidal and bacteriostatic power, minimal tissue toxicity, and blue color, which allows easy visualization of the adhesive in the operative field[4]. On the other hand, cyanoacrylate causes some adverse effects, such as intense inflammation with dissection of the elastic lamina, calcification of the media, and thinning and deformation of the vessel wall. Furthermore, there are accounts of pseudoaneurysm formation and it has been reported that leakage of the glue into the vessel lumen invariably leads to thrombosis[1].
Ideally, a hemostatic agent should be easy to use and conserve, be amiable to sterilization, act only at the site of application, bond quickly to tissue, not release excess heat, be stable at body temperature, maintain adhesiveness even in contact with moist surfaces, only degrade at the final stage of wound healing, be safe for both patient and surgeon, and not have toxicity or carcinogenic action. Unfortunately, an adhesive like this is not yet available[5,6].
It has been demonstrated that vascular sealants, adjuncts to vascular suture, play a major role in reducing operative time, enhancing hemostasis, and reducing the need for additional stitches. Time-honored sealants such as fibrin glue and cyanoacrylate have shown disadvantages in some respects, such as the high cost and intense inflammatory response, respectively[1,3,7].
The aim of the present study was to determine the hemostatic behavior and induced tissue response of bio-based polyurethane derived from castor oil in comparison to 2-octyl-cyanoacrylate following aortic artery injury in guinea pigs.
METHODS
This experimental randomized interventional study was conducted by the Denton Cooley Institute at the histology and cell biology laboratories, the animal colony, and the clinical and surgical experimentation laboratory of the Faculdade Evangélica do Paraná (FEPAR).
Ethical Statement
The Animal Research Ethics Committee (Comitê de Ética em Uso de Animais-CEUA) approved the present study under Formal Opinion No. 5517/2012. The study was conducted in compliance with the ethical principles in animal experimentation adopted by the Brazilian College of Animal Experimentation (Colégio Brasileiro de Experimentação Animal-COBEA) and the regulations laid out in the "Guide for the Care and Use of Laboratory Animals" (Institute of Laboratory Animal Resources, National Academy of Sciences, Washington, D.C., 1996). Moreover, there is no conflict of interest.
Sample Design
The study sample was composed of 24 male guinea pigs (Cavia porcellus), Rodentia, Mammalia, Caviidae, aged 4 months and weighing between 623-882 g (mean, 757.29 g), obtained from the Instituto de Tecnologia do Paraná (TECPAR).
The animals were housed at the FEPAR animal colony in a controlled environment-a room with a low noise level, 12-h light/dark cycles, and mean temperature of 21ºC, varying from 19ºC to 24ºC. The guinea pigs stayed in the animal colony for 30 days prior to the experiment for acclimation and observation. They were kept in cages and received Nuvital chow and water ad libitum[8]. The animals were randomly allocated into three groups of eight animals each[9]: group I (control), group II (polyurethane), and group III (cyanoacrylate).
Group II was subdivided on the basis of the adhesive/catalyst mixture time: 6.5 min for subgroup IIA and 3.5 min for IIB. This difference derived from the homogenization time of polyurethane.
Material
The guinea pigs were purchased from the Institute of Technology of Paraná (TECPAR), while the vascular sealants, polyurethane (Vetasuper®) and 2-octyl-cyanoacrylate (Dermabond®), from processed products.
Surgery Description
After a 6-hour fast for chow and a 4-hour fast for water, the guinea pigs were anesthetized according to the Barzago protocol with ketamine (87 mg/kg) and xylazine (13 mg/kg), intraperitoneally[10]. Abdominal hair was shaved using an electric razor, after which the animals were weighed and tied to the operating board in the supine position. Subsequently, prophylactic enrofloxacin (5-15 mg/kg) was administered intramuscularly. The guinea pigs were wrapped in plastic to prevent hypothermia. Extensive antisepsis with PVPI was done, followed by local anesthesia of the abdominal wall with 2% lidocaine diluted in normal saline (1:4)[11].
We performed median laparotomy with an incision of about 5 cm. The bladder was emptied by puncture with a 13 mm x 0.45 mm needle. The small bowel loops and the descending colon were pushed aside to the right. The ureters were pushed aside and the retroperitoneum was opened. The aorta was dissected from the infrarenal region about 5 mm from the iliac arteries using a small curved hemostat to ensure minimal direct manipulation to minimize vascular injury. Papaverine was applied all around the dissected aorta to prevent vasospasm[12]. The aorta was isolated from the vena cava and clamped using two DeBakey bulldog clamps, proximally and distally to the site being manipulated. We punctured the infrarenal abdominal aorta using a 0.70 mm x 25 mm needle[3]. From this point onward, hemostasis was performed differently for each group. In group I, after puncture of the aorta, the clamps were released and hemostasis was achieved through digital compression with gauze. After it finished bleeding, compression was stopped, restoring blood flow.
In group II, hemostasis was achieved using the bio-based polyurethane sealant in conjunction with a catalyst (at a ratio of 2:1). The mixture was prepared on a sterile slide with varying preparation times as mentioned above. For both subgroups, the sealant was applied at the puncture site using the bare end of a sterile swab stick (Figure 1). To assess the drying time of the adhesive, the proximal clamp was partially released approximately every 15 seconds and blood loss was estimated. After the polyurethane drying process was completed, the DeBakey bulldog clamps were released and arterial blood flow was restored.

For group III, the process began when the capsule containing the 2-octyl-cyanoacrylate adhesive was broken and the product was exposed to air humidity. The adhesive was then placed on a sterile slide. In this group, there was no specific preparation time, since the synthetic adhesive was ready for use in only a few seconds. The technique to apply the cyanoacrylate to the injury site and to assess drying time was identical to that of group II.
To estimate blood loss after the aortic puncture in groups II and III, gauze sponges were weighed on a high-precision scale immediately before they were used and again immediately after. Hemostasis was achieved with sealants; for that reason, the gauze sponges were only used to allow an estimate of blood loss after the puncture and in case of hemostasis failure.
Subsequently, the bowel loops were repositioned without retroperitoneal closure. The abdominal wall was closed in two planes (muscle and skin) with a continuous mononylon 3.0 suture[13].
During the experiment, the following were evaluated: weight of the animal, time of application (puncture of the aorta until the application of sealant), drying time (applying the glue until the opening of the clamps) and blood loss. Except for the weight of the animal, the other variables were analyzed only in groups II and III.
Postoperative period
Postanesthesia recovery took place in a glass box with incandescent light heating, under constant observation of the investigators. After recovery, the animals were returned to their cages. They were given pain medication (5 mg/kg tramadol hydrochloride, intramuscularly) during the first 3 postoperative (PO) days[14].
On PO day 14, the guinea pigs were humanely killed in a CO2 chamber. Following a second median laparotomy, the aorta was surgically removed en bloc from the infrarenal region to about 5 mm from the iliac arteries for histological studies.
Histological Study
The surgical specimens, properly identified, were immersed in 10% formaldehyde for 72 hours at room temperature. The material was routinely processed for slide preparation at the FEPAR histotechnique laboratory. Twelve cuts were made throughout each piece.
The microscope for the histological study was a Nikon Eclipse 200 model. The specimens were analyzed qualitatively and quantitatively at 100x and 400x magnification, respectively.
Fibrous tissue formation was analyzed qualitatively on glass slides using the Masson's trichrome staining technique. Fibrosis was rated as absent/mild or moderate/severe.
In the quantitative analysis with hematoxylin-eosin staining, the cell types were counted in 5 fields under the microscope. The following types were counted: histiocytes, neutrophils, giant cells, and lymphocytes[11].
Statistical Analysis
The results of the quantitative variables were expressed as means, minimum values, maximum values, and standard deviations. The qualitative variables were represented as frequencies and percentages. The nonparametric Mann-Whitney test was used in pairwise comparisons for quantitative variables; comparisons involving more than two groups were made using the nonparametric Kruskal-Wallis test. For the qualitative variables, the groups were compared using Fisher's exact test. Values of P<0.05 indicated statistical significance. The data were analyzed with the aid of the Statistica software, version 8.0.
RESULTS
There were no anesthetic complications. Two animals died postoperatively: 1 in group I on PO day 1 (embolism) and 1 in group III on PO day 2 (evisceration). Given that the deaths occurred in the PO period, we analyzed the intraoperative variables; however, it was not possible to analyze the histological variables, since those animals did not survive through PO day 14.
Group I was only assessed in relation to the weight of the animal and histological variables.
The subdivision of group II was only considered for the intraoperative variables, since this group was judged to be homogeneous for the purposes of the histological study, which assessed the tissue response to the same material across groups.
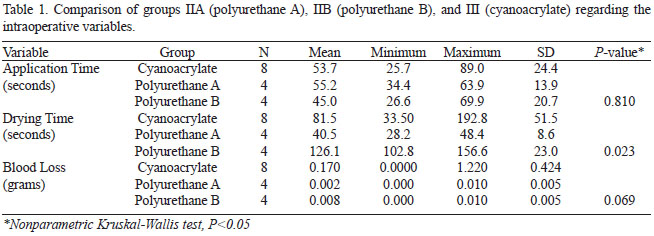
Comparison between groups I, IIA, IIB, and III for intraoperative variables
Application time (seconds): Group IIA (4 animals, mean 55.2, minimum 34.4, maximum 63.9, SD 13.9). Group IIB (4 animals, mean 45.0, minimum 26.6, maximum 69.9, SD 20.7). Group III: (8 animals, mean 53.7, minimum 25.7, maximum 89.0, SD 24.4). There was no statistical significance (P>0.05) among the three groups.
Drying time (seconds): Group IIA (4 animals, mean 40.5, minimum 28.2, maximum 48.4, standard deviation 8.6), Group IIB (4 animals; 126.1 average, minimum 102.8, maximum 156.6, SD 23.0). Group III (8 animals, mean 81.5, minimum 33.5, maximum 192.8, SD 51.5). Drying times were statistically different (P=0.023) among the three experimental groups. In the pairwise comparisons, we observed a trend for a longer drying time in group III relative to group IIA (P=0.069). Group III had a shorter drying time than subgroup IIB (P=0.046); group IIA had a shorter drying time than subgroup IIB (P=0.003).
Blood Loss (grams): Group IIA (4 animals, mean 0.002, minimum 0.000, maximum 0.010, standard deviation 0.005); Group IIB (4 animals, mean 0.008, minimum 0.000, maximum 0.010, standard deviation 0.005); Group III: (8 animals, mean 0.170, minimum 0.000, maximum 1.22, standard deviation 0.424). There was no statistical significance between the three groups (P>0.05).
Descriptive statistics regarding the comparison between groups I, IIA, IIB, and III are shown in Table 1.
Comparison between groups I, II, and III regarding the histological qualitative variable (fibrosis)
Fibrosis was categorized as either absent/mild or moderate/severe on the slides (Table 2).
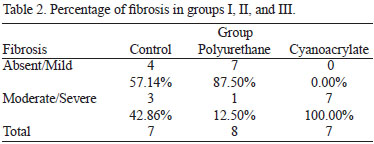
Fibrosis: Group I: absent/mild: 4 (57.14%); moderate/severe: 3 (42.86%). Group II: absent/mild: 7 (87.50%); moderate/severe: 1 (12.50%). Group III: absent/mild: 0 (0.00%); moderate/severe: 7 (100%).
We used pairwise group comparisons to test the null hypothesis that the likelihood of a moderate/severe rating was the same for the two groups compared vs. the alternative hypothesis that the likelihood was different. Group II had statistically less fibrosis than group III (P=0.001), as shown in Figure 2. There was a trend toward increased fibrosis in group III relative to group I (P=0.07). No statistical significance was found between groups I and II.
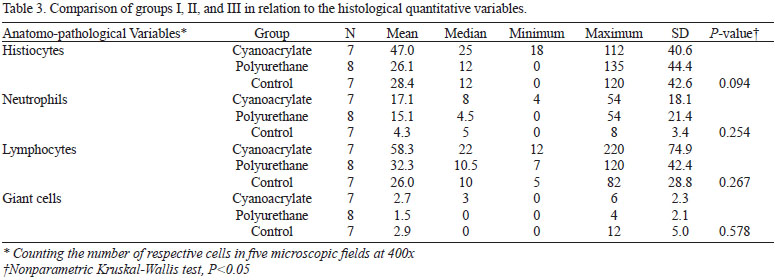
Comparison between groups I, II, and III regarding the histological quantitative variables
For each of these variables, we tested the null hypothesis that the results were equivalent across groups vs. the alternative hypothesis that at least 1 of the groups had different results from the others. The descriptive statistics for the groups and the P-values of the statistical tests are shown in Table 3.
No statistically significant differences were found in the quantitative analysis of the cell types.
DISCUSSION
We chose to work with guinea pigs (Cavia porcellus) because of the small body size of the animal, the ease of handling, and the experience of the research group with this specie.
The choice for 2-octyl-cyanoacrylate was due to our knowledge of several promising studies in cardiovascular surgery such as those of Hall et al.[15], Aziz et al.[16], and Buijsrogge et al.[17]. In addition, this adhesive type is easily accessible-both commercially and financially-compared to other cyanoacrylates for external/internal use (n-butyl-2-cyanoacrylate) or fibrin glue.
In the case of polyurethane, its biocompatibility and mechanical properties (eg, flexibility and adhesiveness) are advantageous; hence, this adhesive is an alternative to the available sealants[11,18]. The currently used polyurethane formulation costs approximately R$ 25.00 (Brazilian Reals) per liter, which would make its use feasible on a large scale. However, for polyurethane to be commercially available as a medical grade product, sterilization processes would be required-and this would raise costs.
The ideal choice for the present experiment regarding hemostasis would be the microvascular suture technique with an adjunctive sealant, as used by Reicher et al.[13], Cho[1], and Ersoy et al.[3]. However, this procedure demands a long learning curve to reduce the risk of anastomotic stenosis, morbidity, and mortality. Therefore, we chose a relatively more simple technique: the aortic puncture, similarly to that described by Ferretti et al.[9].
The intention of the control group was to prove that the diameter of the orifice caused in the aorta was sufficiently large not to stop bleeding spontaneously, requiring a hemostatic method. As the hemostatic technique was different from the other two groups (control had partial blood flow), we did not calculate the surgical time or blood loss.
Therefore, the aim of the intraoperative variables was to compare only IIA, IIB with III, that is, to analyze the efficiency of a sealant known as cyanoacrylate with different preparations of polyurethane.
The drying time was more effective in the cyanoacrylate group (III) compared with the polyurethane B subgroup (IIB), that is, its shorter drying time propitiated quicker hemostasis. However, when group III was compared with subgroup IIA, we noted a trend for polyurethane to be more effective than cyanoacrylate. Considering that the length of time for polyurethane preparation (mixture of adhesive and catalyst) influences drying time, we might have found a statistically significant difference between the hemostatic efficacy of polyurethane vs. cyanoacrylate if the preparation time of the bio-based adhesive were longer than 6.5 minutes. The reason for this is that polyurethane acquires greater adhesiveness with the passing of time after the mixture.
One major advantage of cyanoacrylate is the fact that it is a one-part drying adhesive; thus, it does not require a catalyst, which shortens operative time. One possibility to bring polyurethane closer to this favorable characteristic would be to formulate a novel catalyst or to improve timing in the operating room so that one member of the surgical team would initiate the adhesive mixture only a few minutes before use. The downside of 2-octyl-cyanoacrylate is its short working life (ie, fast preparation). The cyanoacrylate adhesive quickly solidifies after exposed to air humidity, which precludes manipulation if an error leads to a delay in the application of the adhesive. This aspect could entail greater loss of cyanoacrylate in unskilled hands and further raise the costs of the procedure.
In some animals, it was observed by researchers that there was a relatively greater blood loss in group III than in groups IIA and IIB, but without statistical significance. One possible explanation is that cyanoacrylate forms a crust, as noted by Bettes[19] and Fontes et al.[4], and in the event of the crust coming off, massive bleeding would ensue. By contrast, polyurethane, which has elastomeric properties, showed minimally progressive bleeding, thus enabling prompt control of the bleeding.
Radosevish et al.[20], in a review study, stated that cyanoacrylate could lead to extensive fibrosis. Herrera et al.[21] investigated the topical application of cyanoacrylate surrounding previously healthy common carotid arteries in rats-a technique used to strengthen aneurysm walls. Those authors observed intense inflammation, with marked presence of fibroblasts over the first 14 PO days, and moderate presence of fibroblasts at 30 and 60 PO days. The adventitia was found to be thickened due to increased fibrotic connective tissue. In addition, those authors found smooth muscle cell necrosis and rupture of elastic fibers in the media. Gürhan Ulusoy et al.[22] constructed anastomoses with both suture and cyanoacrylate in the femoral artery of rats and, after 21 days, observed periluminal fibroblasts and foreign body giant cells. These works corroborate our findings of enhanced fibrosis at 14 PO days in the 2-octyl-cyanoacrylate group.
Maria et al.[23] reported that the proximal portions of bone grafts of castor-derived polyurethane were covered by fibrotic tissue, with the degree of fibrosis varying between mild, moderate, and severe. Testing the biocompatibility of implants containing polyurethane, Lu et al.[24] affirmed that those prostheses were only partially surrounded by fibrotic tissue. In vascular surgery, Hu et al.[25] demonstrated that, unlike polytetrafluorethylene, which induces marked fibrosis, polyurethane grafts caused fibrosis to a small degree. In our experiment, polyurethane used as a vascular sealant induced significantly less fibrosis than 2-octyl-cyanoacrylate, with a predominance of absent or mild fibrosis.
CONCLUSION
Castor oil-derived polyurethane exhibited a similar hemostatic behavior to that of 2-octyl-cyanoacrylate and showed less intense perivascular tissue response compared to 2-octyl-cyanoacrylate.
REFERENCES
1. Cho AB. Aplicação da cola de fibrina em microanastomoses vasculares: análise comparativa com a técnica de sutura convencional utilizando um modelo experimental de retalho microcirúrgico [Tese de doutorado]. São Paulo: Faculdade de Medicina de São Paulo, 2008. 96p.
2. Freire DF, Taha MO, Soares JH, Simões MJ, Fagundes AL, Fagundes DJ. The laparoscopy splenic injury repair: the use of fibrin glue in a heparinized porcine model. Acta Cir Bras. 2011;26(3):235-41. [MedLine]
3. Ersoy OF, Kayaoğlu HA, Celik A, Ozkan N, Lortlar N, Omeroğlu S. Comparison of cyanoacrylate-assisted arteriotomy closure with conventional closure technique. Ulus Travma Acil Cerrahi Derg. 2009;15(6):535-40. [MedLine]
4. Fontes CER, Taha MO, Fagundes DJ, Ferreira MV, Padro Filho OR, Mardegan MJ. Estudo comparativo do uso de cola de fibrina e cianoacrilato em ferimento de fígado de rato. Acta Cir Bras. 2004;19(1):37-42.
5. Soares Júnior C. Uso de 2-octil cianoacrilato em anastomose colônica: estudo experimental em ratos wistar [Tese de doutorado]. Belo Horizonte: Universidade Federal de Minas Gerais; 2008. 92p.
6. Silva LS, Figueira Neto JB, Santos AL. Utilização de adesivos teciduais em cirurgias. Biosci J. 2007;23(4):108-19.
7. Rocha EAV, Souza C. Avaliação hemodinâmica de anastomoses arteriais reforçadas com selante de fibrina: estudo experimental em suínos. Rev Bras Cir Cardiovasc. 2007;22(1):81-6. [MedLine]
8. Fontes CER, Taha MO, Fagundes DJ, Prado Filho O, Ferreira MV, Mardegan MJ. Estudo do reparo do ferimento de colon com o lado seroso da parede de jejuno, utilizando cianoacrilato e cola de fibrina. Rev Col Bras Cir. 2006;33(2):68-73.
9. Ferretti L, Qiu X, Villalta J, Lin G. Efficacy of BloodSTOP iX, surgicel, and gelfoam in rat models of active bleeding from partial nephrectomy and aortic needle injury. Urology. 2012;80(5):1161.e1-6. [MedLine]
10. Radde GR, Hinson A, Crenshaw D, Toth LA. Evaluation of anaesthetic regimens in guineapigs. Lab Anim. 1996;30(3):220-7. [MedLine]
11. Kubrusly LF, Graça YL, Sucharski EE, Sobral AC, Olandoski M, Kubrusly FB. Biocompatibility of Ricinus comunnis polymer compared to titanium implant used in artificial hearts. Experimental study in guinea pigs. Rev Bras Cir Cardiovasc. 2012;27(3):392-400. [MedLine] View article
12. Santos Junior E, Cividanes GVL, Marchiori RC, Souto FA. Comparação do efeito da nimodipina e da papaverina como vasodilatadores sobre o fluxo na artéria torácica interna esquerda. Rev Bras Cir Cardiovasc. 2006;21(4):403-8. View article
13. Reicher ME, Burihan E, Amorim JE, Nakano LCU, Barros Junior N, Egani MI, et al. Utilização da cola de fibrina em suturas vasculares: aspectos hemodinâmicos. Cir Vasc Angiol. 2001;17(6):195-201.
14. Costa HJZR, Pereira CSB, Costa MP, Fabri FSSS, Lancellotti CLP, Dolci JEL. Estudo experimental comparativo entre o butil-2-cianoacrilato, a mistura gelatina-resorcina-formaldeído e sutura na estabilização de enxertos de cartilagem em coelhos. Rev Bras Otorrinolaringol. 2006;72(1):61-71.
15. Hall WW, Wyre SW, Banducci DR, Ehrlich P. Microvascular anastomosis using 2-octyl cyanoarylate in the rat femoral artery. Ann Plastic Surg. 2000;44(5):508-11.
16. Aziz O, Rahman MS, Hadjianastassiou VG, Kokotsakis J, Vitali M, Cherian A, et al. Novel applications of Dermabond (2-octyl-cyanoacrylate) in cardiothoracic surgery. Surg Technol Int. 2007;16:46-51. [MedLine]
17. Buijsrogge MP, Verlaan CW, Gründeman PF, Borst C. Briefly occlusive coronary anastomosis with tissue adhesive. J Thorac Cardiovasc Surg. 2012;125(2):385-90.
18. Jiang X, Li J, Ding M, Tan H, Ling Q, Zhong Y, et al. Synthesis and degradation of nontoxic biodegradable waterborne polyurethanes elastomer with poly(ε-caprolactone) and poly(ethylene glycol) as soft segment. Eur Polym J. 2007;43(5):1838-46.
19. Bettes PSL. Análise comparativa histológica e tensiométrica entre a cicatrização de feridas cutâneas tratadas com o adesivo octil-2-cianoacrilato e com sutura intradérmica em ratos [Tese de doutorado]. Curitiba: Universidade Federal do Paraná; 2003.
20. Radosevich M, Goubran HI, Burnouf T. Fibrin sealant: scientific rationale, production methods, properties, and current clinical use. Vox Sang. 1997;72(3):133-43. [MedLine]
21. Herrera O, Kawamura S, Yasui N, Yoshida Y. Histological induced oscar changes by aneurysmal in the rat common and carotid coating artery materials wrapping. Neurol Med Chir. 1998;39(2):134-40.
22. Gürhan Ulusoy M, Kankaya Y, Uysal A, Sungur N, Koçer U, Kankaya D, et al. "Lid technique": cyanoacrylate-assisted anastomosis of small-sized vessels. J Plast Reconstr Aesthet Surg. 2009;62(9):1205-9. [MedLine]
23. Maria PP, Padilha Filho JG, Castro MB. Análise macroscópica e histológica do emprego da poliuretana derivada do óleo de mamona (Ricinus communis) aplicada na tíbia de cães em fase de crescimento. Acta Cir Bras. 2003;18(4):332-6.
24. Lu G, Cui SJ, Geng X, Ye L, Chen B, Feng ZG, et al. Design and preparation of polyurethane-collagen/heparin-conjugated polycaprolactone double-layer bionic small-diameter vascular graft and its preliminary animal tests. Chin Med J (Engl). 2013;126(7):1310-6. [MedLine]
25. Hu ZJ, Li ZL, Hu LY, He W, Liu RM, Qin YS, et al. The in vivo performance of small-caliber nanofibrous polyurethane vascular grafts. BMC Cardiovasc Disord. 2012;12:115. [MedLine]
No financial support.
Authors' roles & responsibilities
LFK: Analysis and/or interpretation of data, final approval of the manuscript, conception and design of the study, implementation of operations and/or experiments, manuscript writing or critical review of its content
MSF: Analysis and/or interpretation of data, final approval of the manuscript, conception and design of the study, implementation of operations and/or experiments, manuscript writing or critical review of its content
JVML: Analysis and/or interpretation of data, final approval of the manuscript, conception and design of the study, implementation of operations and/or experiments, manuscript writing or critical review of its content
YLSSG: Conception and design of the study, implementation of operations and/or experiments, manuscript writing or critical review of its content
ACLS: Analysis and/or interpretation of data
MML: Manuscript writing or critical review of its content
Article receive on Saturday, July 12, 2014
 All scientific articles published at rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at rbccv.org.br are licensed under a Creative Commons license



All rights reserved 2017 / © 2025 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()

 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket









