![]()
![]()
Shi-Min Yuan
DOI: 10.5935/1678-9741.20140113
ABSTRACT
OBJECTIVE: A systematic analysis was made in view of the epidemiology, clinical features, diagnosis, treatment and main outcomes of mycobacterial endocarditis.
METHODS: The data source of the present study was based on a comprehensive literature search in MEDLINE, Highwire Press and Google search engine for publications on mycobacterial endocarditis published between 2000 and 2013.
RESULTS: The rapidly growing mycobacteria become the predominant pathogens with Mycobacterium chelonae being the most common. This condition has changed significantly in terms of epidemiology since the 21st century, with more broad patient age range, longer latency, prevailed mitral valve infections and better prognosis.
CONCLUSION: Mycobacterial endocarditis is rare and the causative pathogens are predominantly the rapidly growing mycobacteria. Amikacin, ciprofloxacin and clarithromycin are the most frequently used targeted antimicrobial agents but often show poor responses. Patients with deep infections may warrant a surgical operation or line withdrawal. With periodic multidrug therapy guided by drug susceptibility testing, and surgical managements, patients may achieve good therapeutic results.
RESUMO
OBJETIVO: Uma análise sistemática foi feita considerando epidemiologia, quadro clínico, diagnóstico, tratamento e principais resultados da endocardite micobacteriana.
MÉTODOS: Foi realizada uma pesquisa bibliográfica abrangente no MEDLINE, Highwire Press e no Google para publicações sobre endocardite micobacteriana, publicados entre 2000 e 2013.
RESULTADOS: As micobactérias de crescimento rápido tornam-se os patógenos predominantes, com Mycobacterium chelonae sendo a mais comum. Essa condição se alterou significativamente em termos de epidemiologia, desde o início do século 21, abrangendo faixa etária mais ampla, maior latência, prevalecendo infecções da valva mitral e melhor prognóstico.
CONCLUSÃO: Endocardite micobacteriana é rara e os patógenos causadores são predominantemente as micobactérias de crescimento rápido. Amicacina, ciprofloxacina e claritromicina são os agentes antimicrobianos mais frequentemente utilizados, mas muitas vezes apresentam respostas pobres. Pacientes com infecções profundas podem justificar um procedimento cirúrgico ou retirada de linha. Com a poliquimioterapia periódica guiada por testes de sensibilidade às drogas, e abordagens cirúrgicas, os pacientes podem obter bons resultados terapêuticos.
AVR: Aortic valve replacement
M.: Mycobacterium
MVR: Mitral valve replacement
INTRODUCTION
Cardiac disorders, pregnancy and other surgical maneuvers can be risk factors of bacterial infective endocarditis[1-4]. Increasingly utilization of foreign medical materials, indwelling catheter insertions and intravenous drug uses are recognized risk factors predisposing to bacterial infective endocarditis of the present era[5]. Continuous changes in terms of epidemiology and management strategies of the bacterial infective endocarditis have been elucidated[5]. Staphylococcus aureus has become the most common microorganism of the bacterial infective endocarditis particularly associated with increasing foreign material implant[6], while Streptococcus viridans infections reduced[5]. However, there is no updated elaboration on recent changes of mycobacterial endocarditis.
Mycobacterial endocarditis is rare. It showed a significant predilection of non-tuberculous over tuberculous mycobacteria in terms of infective endocarditis. Due to more resistant to antimicrobial therapies than other pathogens, mycobacteria are often refractory to antimicrobial treatments and are associated with a very high mortality[7]. Rapid-growth non-tuberculous mycobacteria including Mycobacterium (M.) chelonae, M. abscessus and M. fortuitum accounted for 68% of the isolates[8] and thus being the predominant mycobacteria for the infections. There have been systemic reviews on infective endocarditis caused by M. fortuitum[7,9] in 2002, and by M. abscessus[10] and M. chelonae[11] in recent years. Due to the rarity, regular management strategies are still scanty. As for the difficulty of pathogen identifications, poor responses to antimicrobial therapy and poor prognosis, this condition remains a challenge with regard to diagnosis and treatment. However, mycobacterial endocarditis has not been sufficiently elaborated. The present study is designed to highlight the clinical pictures of mycobacterial endocarditis based on relevant literature information published since 2000.
METHODS
MEDLINE, Highwire Press and Google search engine were searched for publications in the English language on mycobacterial endocarditis from 2000 to 2013. The terms "mycobacteria", "heart valve", "heart valve prosthesis", "tuberculous", "non-tuberculous" and "endocarditis" were used for the searches. All the articles, titles and subject headings were screened carefully for potential relevance. Articles were included if the patient had an established diagnosis of mycobacteria endocarditis on current admission and outcome data were reported.
Due to the rarity of the condition, all the discovered articles reported only sporadic single or small series; no large population, comparative studies were retrievable. Therefore, data from this systematic review were qualitatively analyzed as suggested in the Quality of Reporting of Meta-Analyses recommendations.
The search identified 31 relevant studies from 2000 to 2013[7,9-38], including 24 case reports[7,9,10,12,13,15,17-22,24-28,30-33,36-38], 2 case series[14,23], 2 original articles[11,34], 1 medical imaging[16], 1 poster abstract session[29], and 1 "letter to the editor"[35]. After reviewing selected articles, all 31 articles were included and no one was excluded. Data were extracted from the text, figures, or tables and included details of the study population, demographics, types of mycobacteria, sites of infections, locations of vegetations, latency, sensitivity, antimicrobial spectrum, management strategies, clearance time, follow-up length and main outcomes (survivals, complications, relapses, reinterventions and mortality).
Quantitative data were presented as mean±standard deviation, and intergroup differences were compared by unpaired t-test. Comparisons of frequencies were performed by Fisher's exact test. P<0.05 was considered statistically significant.
RESULTS
Demographics
The patient setting included 50 patients with mycobacterial endocarditis. There were 29 males and 21 females with a male-to-female ration of 1.38:1. Their ages were 45.9±19.8 (range, 0.5-78; median 50) years (n=50). Age distribution of the patients conformed to the normal distribution by probability-probability plot.
Clinical features
The major symptoms on admission were described in 46 patients including fever in 35 (76.1%)[7,9-29,33,37,38], dyspnea in 10 (21.7%)[10,11,31,32] and chest pain in 1 (2.1%) patient[30] (χ2=60.7, P=0.000). The duration of the symptoms was 4.0±4.4 (range, 0.17-18; median, 2) months (n=31). The temperature of the febrile patients were 38.9±0.8℃ (n=12). Of the febrile patients, fever grade was not indicated in 22[11,14,18,23,24,26,28,29,33,35,36,38]. In the remaining 13 patients, 5 (38.5%) had a high fever[12,17,19,20,22,29], 5 (38.5%) had a moderate fever[13,15,21,25,34] and 3 (23.1%) had a low-grade fever[9,27,37] (χ2=0.9, P=0.630). Of them, 4 were prolonged fever[24,35,36] and 2 were fever of unknown origin[14,16].
The cardiac murmur was mentioned in 15 patients: a cardiac murmur in 12 (80%) (a pansystolic murmur at the apex in 5[14,21,27,30,38], a diastolic murmur in the aortic region in 2[13,18], a systolic murmur in the aortic region[36], a pansystolic murmur at the apex + a diastolic murmur in the aortic region[25], a pansystolic murmur at the apex + a systolic murmur in the aortic region[15], a systolic murmur at the lower left sternal boarder[37] and an unspecified cardiac murmur[32] in 1 patient each) and an absence of a cardiac murmur in 3 (20%) patients[20,22,24] (χ2=10.8, P=0.001).
Laboratory examinations revealed their hemoglobin was 9.9±1.8 (range, 5.9-12.5; median, 10) g/L (n=10)[9,10,12,13,15,18,20, 27,30,36,38], white blood cell count was 8.9±4.4 (range, 3.3-16.8; median, 8.2) ×109/L (n=13)[9,10,13,15,20-22,24,27,28,30,33,38], platelet count was 165.6±128.7 (range, 67-450; median, 124)×109/L (n=7)[10,13,15,18,20,27,38], C-reaction protein was 6.8±4.7 (range, 0.14-11; median, 8) mg/dL (n=4)[10,20,27,28], and CD4 was 240.5 ± 206.3 (range, 44-587; median 196)/mm3 (n=6)[9,10,13,14,19,37]. CD4 was normal (>500/mm3) in 1 (16.7%) patient, and was abnormal (<500/mm3) in 5 (83.3%) patients (χ2=5.3, P=0.021).
Predisposing risk factors
Cardiac surgery, foreign material implant, intravenous drug use and miscellaneous risk factors were the underlying etiologies for the development of infective endocarditis (χ2=31.9, P=0.000) (Table 1). Of the causative cardiac operations, 23 (85.2%) were heart valve operations and 4 (14.8%) were congenital atrial/ventricular defect patch repairs (χ2=26.7, P=0.000). There were 22 (95.7%) valve replacements and 1 (4.3%) valve repair (χ2 = 38.4, P=0.000). Eighteen (81.8%) were single valve replacements, and 4 (18.2%) were double valve replacements (χ2=17.8, P=0.000); and 17 (77.3%) were first time valve replacements and 5 (22.7%) were redo operations (χ2=13.1, P=0.001). A total of 26 valves were replaced including 13 (50%) aortic and 13 (50%) mitral valve replacements; 20 (80%) were biological, and 5 (20%) were mechanical valve prostheses (χ2 = 18, P=0.000), except the one whose detail of aortic valve prosthesis was not given.
The latency from the presence of the predisposing risk factors to symptom onset was 21.9±25.9 (range, 0.067-96; median, 12) months (n=31)[7,9,11,12,14-18,20,21,23,26,27,31-33,37]. There were 9 (29.0%) early onsets (latency <8 weeks), 2 (6.5%) intermediate onsets (latency was between 8 weeks and 8 months) and 20 (64.5%) late onsets (latency >8 months) (χ2=23.9, P=0.000). The latency of the patients with cardiac operations was much shorter than that of the patients with a foreign material implant, but did not reach a statistical significance (16.4±20.1 months vs. 34.8±39.0 months, P=0.136). It was incompatible with intravenous drug use patients, of which latency was reported in only one patient, and was much shorter than that of the miscellaneity reaching a quasi-statistical difference (16.4±20.1 months vs. 44±34.6 months, P=0.051) (Figure 1). Bioprosthetic valve endocarditis was associated with a longer latency than mechanical without showing a significant difference (17.5±22.5 months vs. 10.8±7.1 months, P=0.569). Four patients had a delayed diagnosis for 0.81±0.24 (range, 0.5-1; median, 0.88) months (n=4)[12,13,20,26].

Infection sites
The infection sites could be divided into 5 types according the location and number of the mycobacterial infections: single intracardiac infection in 38 (76%), two intracardiac infections in 9 (18%), and triple valve infections, single intracardiac + single extracardiac infections, and double intracardiac + single extracardiac infections in 1 (2%) patient, each (χ2=128.5, P=0.000). Including extracardiac infections associated with the endocarditis, totally 64 sites were affected with a mean of 1.28±0.54 (range, 1-3; median, 1) infection sites per patient. There were 1.24±0.48 infection sites in the non-tuberculous and 1.75±0.96 infection sites in the tuberculous endocarditis patients (P=0.067). Native aortic, mitral and tricuspid valves were the most commonly affected sites of mycobacterial endocarditis, representing 29.7%, 26.6% and 10.9%, respectively (Figure 2). No difference was found in the prevalence of infection sites between non-tuberculous and tuberculous mycobacterial endocarditis (Table 2), or in the strain distributions between aortic and mitral valves (Table 3).

Vegetations were detected in 44 patients with 43 detected by echocardiography and 1 patient detected by positron emission tomography with 18F-fluorodeoxyglucose uptake[16]. Of them, 12 (27.3%) patients did not have a visualized vegetation[7,9,11,14,17,28,31], but one of them with an abscess along the inferior and septal walls, instead[31] and 32 (72.7%) patients had (χ2=18.2, P=0.000). The vegetation locations of the remaining 32 patients were mitral valve in 10 (31.3%)[11,20,21,30,36,37] (two of them were in the prosthetic mitral valve)[20,21], aortic valve in 7 (21.9%)[11,13,18,32,33,38] (one was in the prosthetic aortic valve)[33], pacemaker lead in 3 (12.5%)[16,26,27], tricuspid valve in 3 (9.4%)[10,19,35], both mitral valve and right subclavian catheter in 1 (3.1%)[36], both mitral and aortic valves in 2 (6.3%)[12,15], both aortic and tricuspid valves in 2 (6.3%)[22,24], mitral, aortic and tricuspid valves in 1 (3.1%)[25], tricuspid valve and ventricular septal defect patch in 2 (6.3%)[35] and atrial septal patch in 1 (3.1%) patient[23], respectively. The detection time for a positive vegetation was described in 3 patients, which was 5[13], 21[20] and 105 days[15] after admission, respectively. Dimensions of the vegetations were recorded in 16 patients for 17 vegetations. Five vegetations of 5 patients from a single report[11] were recorded as "minimal", which were excluded from the calculation of the vegetation size. The size of the remaining 12 vegetations of 11 patients was 19.7±18.4 (range, 5-70; median, 15.5) mm[10,15,18,20,23-26,30,32,37]. Valve insufficiency was present in 23 (46%) patients: mitral valve regurgitation in 9 (39.1%)[11,30,31,37] (6 were prosthetic mitral valve leaks[11]), aortic valve regurgitation in 5 (21.7%)[11,28,32] (4 were prosthetic aortic valve leaks[11,32]), aortic and mitral valve regurgitation in 5 (21.7%)[11,12,14,38] (2 were prosthetic aortic and mitral valve leaks[11]) and tricuspid valve regurgitation in 4 (17.4%) patients[10,27,35]. There were totally 11 (47.8%) native valve regurgitations and 12 (52.2%) prosthetic valve leaks (χ2=0.1, P=0.768). Besides, one patient had inferior and septal wall abscess associated with mitral valve regurgitation[31] and one patient had ventricular septal patch dehiscence[35].
Pathogens
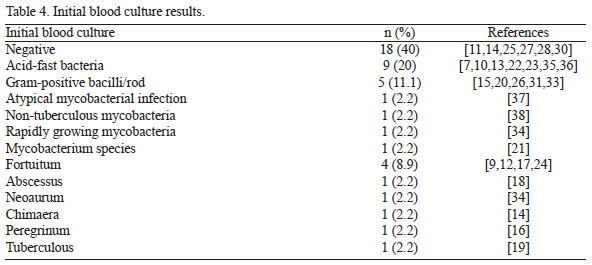
The initial blood culture results were not indicated in 5 patients[29,34]. In the remaining 45 patients, a negative culture prevailed, followed by an acid-fast bacterium (Table 4).
Thirty-seven patients had more investigations performed for strain identifications. Fourteen patients had more samples than blood for cultures: 7 (50%) patients had one more sample, 4 (28.6%) patients had 2 more samples, 2 (14.3%) patients had 3 more samples and 1 (7.1%) patient had 4 more samples for cultures, respectively. There were totally 25 additional samples for cultures including 4 (16%) intraoperative excised valves[12,18], or valve prosthesis[7], or prosthetic valve ring[14], 4 (16%) resected vegetations[27,30,35], 3 (12%) sputum[27,28,34], 2 (8%) bronchoalveolar lavage[14,27], 2 (8%) urine[14,27], 2 (8%) bone marrow[14,37], 1 (4%) removed patch[35], removed pacing lead[26], intraoperative specimens (with no details available)[34], pacemaker generator pocket site[26], aspirated fluid[26], sternum[7], cerebrospinal fluid[37] and tracheal swab[15] for each, respectively. Lowenstein-Jensen medium was once used for valve, sternum and blood cultures[7]. Three (12%) were negative and 22 (88%) were positive (χ2=28.8, P=0.000). The 22 positive cultures identified the strains to be M. fortuitum in 7 (31.8%), M. chimaera in 4 (18.2%), M. abscessus in 3 (13.6%), M. chelonae in 2 (9.1%), M. neoaurum in 1 (4.5%), acid-fast bacilli in 2 (9.1%), rapidly growing mycobacteria in 1 (4.5%) and tubercule bacilli in 2 (9.1%), respectively. At least 15 (68.2%) cases were rapid growing mycobacteria infections.
Seventeen patients (four of them had additional samples for cultures) had a positive histological staining results by Ziehl-Neelsen and auramine-rhodamine stains[12,17,18,27] with acid-fast organisms shown on fluorescence microscopy.
Ten patients had a molecular analysis of the mycobacteria, where 16s ribosomal deoxyribonucleic acid sequencing was applied in 4 (40%)[14,20,21,23], reverse line blot hybridization in 4 (40%)[29] and a polymerase chain reaction-restriction fragment length polymorphism analysis in 2 (20%) patients [10,33], respectively. All patients had fresh samples, and one of them had additional cryopreserved samples for investigations. However, analyses on the cryopreserved samples disclosed negative results, while all fresh specimens displayed positive results. In addition, two patients had mycolic acid analysis by biochemical and chromatographic techniques[7,9].
By preliminary blood cultures, histological staining, molecular analyses and chromatographic techniques, the eventual mycobacterial strains were identified in all but one patient (Figure 3). Distributions of the mycobacteria responding to the four predisposing risk factors showed cardiac operation was associated with more, prevailed rapidly growing mycobacteria (M. chelonae, M. fortuitum and M. chimaera) endocarditis, foreign material implant was associated with M. fortuitum, and intravenous drug use and miscellaneity were prone to be of tuberculous endocarditis (Figure 4, Table 5).


According to the antimicrobial spectrum, intravenous amikacin 300 mg twice daily, ciprofloxacin 400-500 mg twice daily and clarithromycin 500 mg twice daily were the most frequently used targeted antimicrobial agents, and imipenem (500 mg/6 hours), linezolid, rifampicin and trimethoprim/sulfamethoxazole 160 mg/800 mg (p.o., thrice daily) were more frequently used for non-tuberculous mycobacterial infection; while ethambutol (20 mg/kg/day), isoniazid (10 mg/kg/day), pyrazinamide (25 mg/kg/day) and rifampicin (10 mg/kg/day) were for tuberculous mycobacterial infection. The antimycobacterial course was life in 2 patients[18,35]. In another 19 patients[10-13,22-24,26,28,33,34], the treatment course was indicated, which was 2.7±2.3 (range, 0.83-9; median, 1.67) months. The clearance time interval was 31.8±58.4 (range, 2-210; median, 12.5) days (n=12)[12,13,15,19-21,23,34,35].
Prognosis
Patients were at a follow-up of 48.7±39.8 (range, 3-116; median, 32) months (n=23)[9,11,17,19-21,23,26,30,32,34]. Totally 27 (50%) patients were event-free survivals[12,16,17,19,20,22-24,26,28,30,33-35], 3 (6.25%) patients relapsed at 0.5, 5 and 10 months, respectively[9,10,18], 4 (6.25%) patients were complicated[21,25,29,32] and one of them required reintervention[32], which constituted the only reintervention of the whole setting, and 17 (34%) patients died[11-15,18,27,29,31,36-38] at 83.9±85.9 (range, 1-270; median, 64) days (n=11). The death causes were described in 8 patients, which were multiorgan failure in 2[12,15], and candidaemia and hospital-acquired pneumonia[36], persistent mycobacteremia and stroke[29], progressive heart failure[14], respiratory distress[37], splenic rupture[14] and variceal bleeding[31] in 1 patient, each.
Two patients did not receive either medical or surgical treatment, but had a good prognosis in each. Of the remaining 48 patients, 32 (66.7%) patients received an antimicrobial therapy alone, 10 (20.8%) patients had a cardiac operation and 6 (12.5%) patients had an intervention for removal of catheter/lead/defibrillator (χ2=36.8, P=0.000).
In the patients with medical treatment, there were 17 event-free survivals[11,19,22,30,34,35], 11 deaths[11,13,14,29,31,37,38], 2 complicated (spleen infarct, renal infarct and cerebral abscess on day 10, and prosthetic valve endocarditis due to coagulase negative staphylococcal species at 1 year in one patient[21]; and periaortic abscess in another[29]) and 2 relapses[9,10]. In the surgical treatment group, all patients received a valve replacement operation, including 2 aortic valve replacements (AVRs), 1 AVR with root replacement, 1 redo-AVR, 1 2nd redo-AVR, 2 AVRs + mitral valve replacements (MVRs), 1 AVR + MVR + tricuspid valvuloplasy, 1 2nd redo-AVR + MVR and 1 redo-MVR. There were 5 event-free survivals[12,17,20,28,33], 3 deaths[12,18,29], 2 complicated (1 preoperative stroke and 1 complication related with his previous ascending aortic replacement)[25,32], 1 relapse[18] and 1 reintervention[32]. In the patients with a catheter/lead/defibrillator removal, there were 3 event-free survivals[16,24,26] and 3 deaths[15,27,36]. Time of deaths was described in 11 patients. There were 4 (36.4%) early deaths and 7 (63.6%) late deaths (χ2=1.6, P=0.201).
DISCUSSION
In 1959, Runyon[39], according to pigment of colony and rate of growth, divided mycobacteria into 4 types: photochromogen, scotochromogen, nonphotochromogen and rapid grower. The latter one, rapidly growing mycobacterium, was defined so because the mycobacterial colonies form at 25-45&ºC on solid agar in 5-7 days. Both slowly and rapidly growing mycobacteria are environmental opportunistic mycobacteria that are normal inhabitants of natural waters, drinking water and soils[40]. The most important slowly growing species are M. avium and M. intracellulare, called the M. avium complex; and rapidly growing mycobacteria (M. abscessus, M. chelonae and M. fortuitum), which are opportunistic pathogens[40].
Mycobacterial endocarditis is rare. In a recent report of infective endocarditis incorporating information from 13 tertiary hospitals in Turkey, no myocabacterial endocarditis was reported[41]. Wallace et al.[42] stated that the incidence of mycobacterial endocarditis was 33.3% (4/12) out of M. fortuitum or M. chelonae bacteria and was 3.2% of rapid growth mycobacterial blood infections. Olalla et al.[7] reviewed 19 cases of rapid growth mycobacterial endocarditis and noted that patients' age was 45 (range, 20-74) years, including 4 native and 15 prosthetic valve endocarditis, with a biological valve prosthesis in 6 and a mechanical valve prosthesis in 9 patients.
The degree of fever may not correspond to the severity of the illness[43]. As it was illustrated in the present article, no dominance of fever grade was associated with mycobacterial endocarditis. Strabelli et al.[11] reported that the latent for the febrile onset and development of valve dysfunction was few days and months to years, respectively. In 5 of 13 patients with prosthetic mycobacterial endocarditis, the latent period for the diagnosis of bioprosthetic endocarditis was 1-4 years[11]. Olalla et al.[7] reported a latency of 12 weeks from infection to symptom onset with no difference found between biological and mechanical prosthetic valve endocarditis. The present study revealed a more broad patient age range from infant to 78 years old with a normal age distribution, equality of affected aortic and mitral valves, more native than prosthetic valve and more bioprosthetic than mechanical bioprosthetic endocarditis. Moreover, cardiac operations caused a shorter latency to endocarditis occurrence than foreign material implant and miscellaneous risk factors. Bioprosthetic valve endocarditis was associated with a longer latency than mechanical but lack of a significant difference. Kunin et al.[9] reported a prevailed early onset of mycobacterial endocarditis. Valve dysfunction was noted in 10 (76.9%) patients, while only 3 (23.1%) patients were free of valve dysfunction (χ2=12.5, P=0.001). The present study demonstrated a predominant late onset and a decreased incidence of valve dysfunction.
The most common predisposing risk factors for mycobacterial infections include medical procedures (central venous access, hemodialysis catheter indwelling, various surgical operations including mammoplasty, arthroplasty and cardiothoracic operations)[9], immunocompromised, particularly patients with human immunodeficiency virus/acquired immunodeficiency syndrome, hematological malignancies, or those treated with immunosuppressive drugs after solid organ transplantation[44]. More recently, the use of tumor necrosis factor-αblockers has become an additional risk factor[45]. Line-related non-tuberculous infections did not have any predominant organisms including M. abscessus, M. chelonae, M. neoaurum, M. fortuitum and M. mucogenicum[34]. Further, possible manufacturer contamination of bioprosthesis by M. chelonea has been recognized[46]. In addition, nosocomial infections were once evidenced from sources like cardioplegic solutions[47], water supply[48], antiseptic solutions[49] and valve prosthesis preservation solutions[50].
Positivity of blood cultures varied according to types of affected valves. It was 75% in mechanical, 20% in biological and 100% in native valves[7]. Removed valve prostheses showed a high positivity of mycobacterial cultures[48]. Upon colonial growth, gram and acid-fast stains should be performed, and then when blood cultures are negative, acid-fast bacilli stains on histological examination of the removed prosthetic valves[11] and Ziehl-Neelsen stain should be employed, followed by subcultures[40].
Mycobacteria are more resistant to chemical disinfection than other pathogens[11]. Infective endocarditis caused by rapidly growing mycobacteria is always refractory due to extensive drug resistance and substantially delayed diagnosis[36]. The poor response to therapy can be a result of various factors that may lead to drug resistance, including the presence of biofilms, type of antimicrobial agent used and presence of a novel inducible erm(41) gene[51]. With periodic multidrug therapy guided by drug susceptibility testing, patients may achieve good therapeutic results[51]. Therefore, antimicrobial susceptibility tests of the isolates are of important clinical significance[36]. The management of rapidly growing mycobacteria is usually an empiric therapy with two agents and a successive targeted regimen according to drug sensitivity tests[9]. Amikacin was the most reliable agent for the treatment of non-tuberculous mycobacteria and alternative effective agents included ciprofloxacin, clarithromycin, imipenem and linezolid[34]. Non-tuberculous mycobacteria are more sensitive to some antibiotics than other rapidly growing mycobacteria[32]. Clarithromycin was proved to be sensitive to M. abscessus/chelonae. Moxifloxacin was discovered to be the best to treat M. fortuitum infections, very active against M. chelonae when used alone and more effective against all the strains when combined with clarithromycin and amikacin[52]. A combined use of clarithromycin with moxifloxacin or linezolid at a high concentration (16 μg/ml) also displayed activity against M. abscessus[51]. Disseminated infections with atypical mycobacteria often develop in immunocompromised patients with reduced CD4 count and complement levels[37]. A combined antimicrobial therapy with prolonged treatment duration is often the regimen of choice. Amikacin and imipenem have been proved to be effective agents for the disseminated cases[32].
Patients with deep infections of rapidly growing mycobacteria often warrant a surgical intervention including line removal, debridement, or removal of the foreign material[34]. An improved survival was advocated to be associated with surgical interventions[33], whereas some patients with conservative managements failed to survive[13]. In the patient series of Olalla et al.[7] reported in 2002, 15 of 19 cases of M. fortuitum complex (M. fortuitum and M. chelonae) endocarditis were prosthetic valve endocarditis and valve replacement was performed in 8 (42.1%) patients with an overall mortality of 88%. Recently, Strabelli et al.[11] reported 13 patients with M. chelonae endocarditis received a valve replacement and an overall mortality was decreased to 23.1% (3/13) including 1 (7.7%) early and 2 (15.4%) late deaths. Exceptionally, a few patients did not receive any antimicrobial treatment and patients were at long-term event-free survival[11]. These results implied that foreign material implant becomes an apparent risk factor for infective endocarditis, and usage of higher dose and combined antimicrobial regimens with reference to the mycobacterial species and surgical treatment can lead to improved outcomes.
The rarity of this condition as well as the relevant published materials made this study a limited patient population. Abundant valuable date in the future may replenish the research with more accurate results.
CONCLUSION
Mycobacterial endocarditis is rare but dreadful. The rapidly growing mycobacteria become the predominant pathogens with chelonae being the most common. This condition has changed significantly in terms of epidemiology since the 21st century, with more broad patient age range, longer latency, prevailed mitral valve infections and better prognosis. The better prognoses than before might be attributed to the faster strain identification molecular techniques, higher dose of antimicrobial agents, periodic multidrug therapy guided by drug susceptibility testing and more requirements of surgical interventions.
REFERENCES
1. Yuan SM, Demesthenous E, Coman V. Long QT syndrome in extensive infective endocarditis complicating hypertrophic obstructive cardiomyopathy. Kardiol Pol. 2009;67(1):53-7. [MedLine]
2. Yuan SM, Jing H. The bicuspid aortic valve and related disorders. Sao Paulo Med J. 2010;128(5):296-301. [MedLine]
3. Yuan SM, Wu B, Hu XN, Jing H. Axillary artery thrombus and infective endocarditis in lupus. J Chin Med Assoc. 2011;74(1):40-3. [MedLine]
4. Al Jama PE. Obstetric outcome of teenage pregnancies: a 5-year experience in a university hospital. Kuwait Med J. 2012;44:195-9.
5. Yuan SM. Right-sided infective endocarditis: recent epidemiologic changes. Int J Clin Exp Med. 2014;7(1):199-218. [MedLine]
6. Vaccarino GN, Nacinovich F, Piccinini F, Mazzetti H, Segura E, Navia D. Pacemaker endocarditis: approach for lead extraction in endocarditis with large vegetations. Rev Bras Cir Cardiovasc. 2009;24(4):570-3. [MedLine] View article
7. Olalla J, Pombo M, Aguado JM, Rodríguez E, Palenque E, Costa JR, et al. Mycobacterium fortuitum complex endocarditis-case report and literature review. Clin Microbiol Infect. 2002;8(2):125-9. [MedLine]
8. Matos ED, Santana MA, de Santana MC, Mamede P, de Lira Bezerra B, Panão ED, et al. Nontuberculosis mycobacteria at a multiresistant tuberculosis reference center in Bahia: clinical epidemiological aspects. Braz J Infect Dis. 2004;8(4):296-304. [MedLine]
9. Kunin M, Salamon F, Weinberger M, Genkin I, Sagie A, Tur-Kaspa R. Conservative treatment of prosthetic valve endocarditis due to Mycobacterium fortuitum. Eur J Clin Microbiol Infect Dis. 2002;21(7):539-41. [MedLine]
10. Tsai WC, Hsieh HC, Su HM, Lu PL, Lin TH, Sheu SH, et al. Mycobacterium abscessus endocarditis: a case report and literature review. Kaohsiung J Med Sci. 2008;24(9):481-6. [MedLine]
11. Strabelli TM, Siciliano RF, Castelli JB, Demarchi LM, Leão SC, Viana-Niero C, et al. Mycobacterium chelonae valve endocarditis resulting from contaminated biological prostheses. J Infect. 2010;60(6):467-73. [MedLine]
12. Collison SP, Trehan N. Native double-valve endocarditis by Mycobacterium fortuitum following percutaneous coronary intervention. J Heart Valve Dis. 2006;15(6):836-8. [MedLine]
13. Spell DW, Szurgot JG, Greer RW, Brown JW 3rd. Native valve endocarditis due to Mycobacterium fortuitum biovar fortuitum: case report and review. Clin Infect Dis. 2000;30(3):605-6. [MedLine]
14. Achermann Y, Rössle M, Hoffmann M, Deggim V, Kuster S, Zimmermann DR, et al. Prosthetic valve endocarditis and bloodstream infection due to Mycobacterium chimaera. J Clin Microbiol. 2013;51(6):1769-73. [MedLine]
15. Al-Benwan K, Ahmad S, Mokaddas E, Johny M, Kapoor MM. Diagnosis of endocarditis caused by Mycobacterium abscessus. Ann Saudi Med. 2010;30(5):408-11. [MedLine]
16. Amraoui S, Texier-Maugein J, Bordachar P. PET scan in suspected but unproven pacemaker endocarditis. Arch Cardiovasc Dis. 2012;105(2):125-6. [MedLine]
17. Bosio S, Leekha S, Gamb SI, Wright AJ, Terrell CL, Miller DV. Mycobacterium fortuitum prosthetic valve endocarditis: a case for the pathogenetic role of biofilms. Cardiovasc Pathol. 2012;21(4):361-4. [MedLine]
18. Corrales-Medina V, Concha R, Simkins J, Sanchez M, Baracco G. Native valve endocarditis caused by rapidly growing mycobacteria: case report and review of the literature. Scand J Infect Dis. 2007;39(6-7):639-41. [MedLine]
19. Fumagalli J, Bonifacio C, Gulotta H, Shinzato R, Troncoso A. Bacterial endocarditis: a role for Mycobacterium tuberculosis? AIDS. 2002;16(13):1845-6. [MedLine]
20. Jönsson G, Rydberg J, Sturegård E, Christensson B. A case of Mycobacterium goodii prosthetic valve endocarditis in a non-immunocompromised patient: use of 16S rDNA analysis for rapid diagnosis. BMC Infect Dis. 2012;12:301. [MedLine]
21. Kumar A, Pazhayattil GS, Das A, Conte HA. Mycobacterium neoaurum causing prosthetic valve endocarditis: a case report and review of the literature. Braz J Infect Dis. 2014;18(2):235-7. [MedLine]
22. Natsag J, Min Z, Hamad Y, Alkhalil B, Rahman A, Williams R. A mysterious gram-positive rods. Case Rep Infect Dis. 2012;2012:841834. [MedLine]
23. Sadanandan R, Kuriakose KM, Ramanarayanan PV, Philomina B. Mycobacterium massiliense: an emerging pathogen in cardiovascular infections. Asian Cardiovasc Thorac Ann. 2013;21(1):77-8. [MedLine]
24. Shah P, Vishnevsky A. Mycobacterium fortuitum device infection with subsequent endocarditis. Med Forum 2012;13:Article 13 [Accessed Apr 5 2014]. Available at: http://jdc.jefferson.edu/tmf/vol13/iss1/13
25. Shaikh Q, Mahmood F. Triple valve endocarditis by mycobacterium tuberculosis: a case report. BMC Infect Dis. 2012;12:231. [MedLine]
26. Sharma S, Tleyjeh IM, Espinosa RE, Costello BA, Baddour LM. Pacemaker infection due to Mycobacterium fortuitum. Scand J Infect Dis. 2005;37(1):66-7. [MedLine]
27. Sharma H, Keshavan A, Little MA, Cross J, Lipman MC, Talukdar S, et al. Fortuitous vasculitis. Ren Fail. 2012;34(3):378-82. [MedLine]
28. Sogabe O, Ohya T. A case of tuberculous endocarditis with acute aortic valve insufficiency and annular subvalvular left ventricular aneurysm. Gen Thorac Cardiovasc Surg. 2007;55(2):61-4. [MedLine]
29. Soman R, Gupta N, Shetty A, Rodrigues C. 1732. Prosthetic endocarditis due to nontuberculous Mycobacteria: a new problem in the developing world. Session: Poster Abstract Session: Tuberculosis and other Mycobacterial Infections. Saturday, October 20, 2012. Room: SDCC Poster Hall F-H [Accessed Apr 5 2014]. Available at: https://idsa.confex.com/idsa/2012/webprogram/Paper35271.html
30. Sultan FA, Fatimi S, Jamil B, Moustafa SE, Mookadam F. Tuberculous endocarditis: valvular and right atrial involvement. Eur J Echocardiogr. 2010;11(4):E13. [MedLine]
31. Takekoshi D, Al-Heeti O, Belvitch P, Schraufnagel DE. Native-valve endocarditis caused by Mycobacterium chelonae, misidentified as polymicrobial gram-positive bacillus infection. J Infect Chemother. 2013;19(4):754-6. [MedLine]
32. Torres-Duque CA, Díaz C, Vargas L, Serpa EM, Mosquera W, Garzón MC, et al. Disseminated mycobacteriosis affecting a prosthetic aortic valve: first case of Mycobacterium peregrinum type III reported in Colombia. Biomedica. 2010;30(3):332-7. [MedLine]
33. Vail G, Kohler R, Steiner F, Donepudi R. Successful treatment of Mycobacterium fortuitum prosthetic valve endocarditis: case report. Clin Infect Dis. 2000;30(3):629-30. [MedLine]
34. van Duin D, Goldfarb J, Schmitt SK, Tomford JW, Tuohy MJ, Hall GS. Nontuberculous mycobacterial blood stream and cardiac infections in patients without HIV infection. Diagn Microbiol Infect Dis. 2010;67(3):286-90. [MedLine]
35. Vuković D, Parezanović V, Savić B, Dakić I, Laban-Nestorović S, Ilić S, et al. Mycobacterium fortuitum endocarditis associated with cardiac surgery, Serbia. Emerg Infect Dis. 2013;19(3):517-9. [MedLine]
36. Williamson JC, Miano TA, Morgan MR, Palavecino EL. Fatal Mycobacterium abscessus endocarditis misidentified as Corynebacterium spp. Scand J Infect Dis. 2010;42(3):222-4. [MedLine]
37. Liebeskind DS, Ostrzega N, Wasterlain CG, Buttner EA. Neurologic manifestations of disseminated infection with Mycobacterium abscessus. Neurology. 2001;56(6):810-3. [MedLine]
38. Jagadeesan N, Patra S, Singh AP, Nagesh CM, Reddy B, Badnur SC, et al. Spontaneous endocarditis caused by rapidly growing non-tuberculous Mycobacterium chelonae in an immunocompetent patient with rheumatic heart disease. J Cardiovasc Dis Res. 2013;4(4):254-6. [MedLine]
39. Runyon EH. Anonymous mycobacteria in pulmonary disease. Med Clin North Am. 1959;43(1):273-90. [MedLine]
40. Falkinham JO 3rd. Nontuberculous mycobacteria in the environment. Clin Chest Med. 2002;23(3):529-51. [MedLine]
41. Elbey MA, Akdağ S, Kalkan ME, Kaya MG, Sayın MR, Karapınar H, et al. A multicenter study on experience of 13 tertiary hospitals in Turkey in patients with infective endocarditis. Anadolu Kardiyol Derg. 2013;13(6):523-7. [MedLine]
42. Wallace RJ Jr, Swenson JM, Silcox VA, Good RC, Tschen JA, Stone MS. Spectrum of disease due to rapidly growing mycobacteria. Rev Infect Dis. 1983;5(4):657-79. [MedLine]
43. Tunkel AR. Fever in adults [Accessed Apr 5 2014]. Available at: http://www.merckmanuals.com/home/infections/biology_of_infectious_disease/fever_in_adults.html
44. van Ingen J. Diagnosis of nontuberculous mycobacterial infections. Semin Respir Crit Care Med. 2013;34(1):103-9. [MedLine]
45. Winthrop KL, Chang E, Yamashita S, Iademarco MF, LoBue PA. Nontuberculous mycobacteria infections and anti-tumor necrosis factor-alpha therapy. Emerg Infect Dis. 2009;15(10):1556-61. [MedLine]
46. Tyras DH, Kaiser GC, Barner HB, Laskowski LF, Marr JJ. Atypical mycobacteria and the xenograft valve. J Thorac Cardiovasc Surg. 1978;75(3):331-7. [MedLine]
47. Wallace RJ Jr, Musser JM, Hull SI, Silcox VA, Steele LC, Forrester GD, et al. Diversity and sources of rapidly growing mycobacteria associated with infections following cardiac surgery. J Infect Dis. 1989;159(4):708-16. [MedLine]
48. Kuritsky JN, Bullen MG, Broome CV, Silcox VA, Good RC, Wallace RJ Jr. Sternal wound infections and endocarditis due to organisms of the Mycobacterium fortuitum complex. Ann Intern Med. 1983;98(6):938-9. [MedLine]
49. Fraser DW. Bacteria newly recognized as nosocomial pathogens. Am J Med. 1981;70(2):432-8. [MedLine]
50. Laskowski LF, Marr JJ, Spernoga JF, Frank NJ, Barner HB, Kaiser G, et al. Fastidious mycobacteria grown from porcine prosthetic-heart-valve cultures. N Engl J Med. 1977;297(2):101-2. [MedLine]
51. Jarand J, Levin A, Zhang L, Huitt G, Mitchell JD, Daley CL. Clinical and microbiologic outcomes in patients receiving treatment for Mycobacterium abscessus pulmonary disease. Clin Infect Dis. 2011;52(5):565-71. [MedLine]
52. Cremades R, Santos A, Rodríguez JC, García-Pachón E, Ruiz M, Escribano I, et al. Screening for sterilizing activity of antibiotic combinations in an acid model of rapidly growing mycobacteria during the stationary phase of growth. Chemotherapy. 2009;55(2):114-8. [MedLine]
No financial support.
Authors' roles & responsibilities
SMY: Main Author
Article receive on Thursday, April 24, 2014
 All scientific articles published at rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at rbccv.org.br are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()




 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket