![]()
![]()
Hui WuI; Weiyu ChangI; Yanglin DengI; Xinli ChenI; Yongli DingI; Xuesong LiI; Liang DongII
DOI: 10.21470/1678-9741-2018-0306
ABSTRACT
Objective: To study the response of myocardial ischemia/reperfusion injury (MI/RI) in rats to simulated geomagnetic activity.CK = Creatine kinase
cTnI = Troponin I
ELISA = Enzyme-linked immunosorbent assay
LAD = Left anterior descending
LDH = Lactate dehydrogenase
LEVDP = Left ventricular end-diastolic pressure
LVDP = Left ventricular developed pressure
MI = Myocardial ischemia
RI = Reperfusion injury
SPSS = Statistical Package for the Social Sciences
TTC = Triphenyl tetrazolium chloride
INTRODUCTION
The Earth's magnetic field is a protective barrier to life. The growth, development, and migration of living things require this magnetic field. Human activities are inextricably linked to the Earth's magnetic field as well. At present, about 3.5 million people die of cardiovascular and cerebrovascular diseases each year in China, accounting for over 40% of the total number of deaths due to various causes[1]. Studies have shown that the occurrence and development of cardiovascular and cerebrovascular diseases are closely related to the geomagnetic field, but the specific mechanism of influence is not yet clear[2,3]. The traditional research methods can't explain the mechanism of geomagnetic activity on cardiovascular and cerebrovascular diseases. Therefore, this project intends to simulate geomagnetic activity and study the response of myocardial ischemia/reperfusion injury (MI/RI) in rats to this geomagnetic activity. It will provide a new way to study the relationship between geomagnetic activities and cardiovascular diseases. And the results of this study can provide a new idea to treat the patients with MI/RI, when there is a geomagnetic outbreak.
METHODS
Animal and Ethical Statement
The present study used eight to ten-week-old male Sprague-Dawley rats (Charles River), weighing 200±20 g, which were obtained from the Experimental Animal Center of the Kunming Medical University (Kunming, Yunnan, China) and were housed in the Laboratory Animal Center of the Kunming Medical University. Animal experimental protocols were approved and performed according to the guidelines of the Institutional Medical Experimental Animal Care Committee of the Kunming Medical University. Guidelines for Laboratory Animal Care and Safety from the United States National Institutes of Health (Bethesda, Maryland, USA) were also followed.
Reagents
Triphenyl tetrazolium chloride (TTC) was obtained from the Sigma-Aldrich Corporation (Missouri, USA). Kits for detecting lactate dehydrogenase (LDH), creatine kinase (CK), and troponin I (cTnI) were purchased from AU Clinical Chemistry Systems of the Beckman Coulter Inc. company (California, USA). The kit for detecting melatonin was purchased from the Abcam Inc. company (ab213978, Abcam, Cambridge, Massachusetts, USA).
Equipment
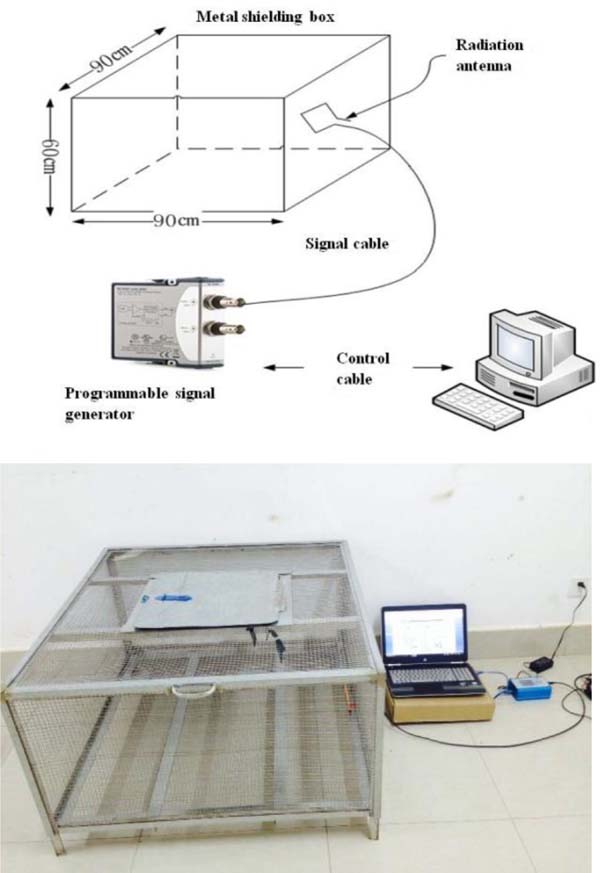
The geomagnetic experimental platform consists of four partial compositions, including a metal shielding experiment cage, radiation antenna, programmable signal generator, and control computer. The signal generator controlled by the main control computer can produce below 50 Hz and an arbitrary combination of signal spectra, especially analog Schumann resonances and geomagnetic burst, in the space of electromagnetic radiation (Figure 1). Patent No.: ZL201520208744.2.
Animal Grouping and Treatment
The male rats were randomly divided into the geomagnetic shielding place, geomagnetic radiation place, and normal place (rats living in general environment without intervention). The rats in each place were divided into sham operation group and operation group, being nine rats in each group. The shield+sham group, radiation+sham group, normal+sham group, and normal+operation group were the control group. The shield+operation group and radiation+operation group were the experimental group.
MI/RI Protocol
The MI/RI model was generated and utilized as previously described[4,5]. Rats were anesthetized using an intraperitoneal injection of 3.6% chloral hydrate (1 ml/kg) and ventilated isoflurane gas via tracheal intubation, with an RWD rodent respirator. Body temperature was maintained at 37ºC via a heated operating table. MI/RI surgery was performed using the following procedure: the heart was exteriorized by a left thoracic incision, and a slipknot (6-0 silk) was placed and ligated around the left anterior descending (LAD) coronary artery. The slipknot was released after 30 min of ischemia, and after that the animal received 24 hours of reperfusion. Ischemia was confirmed by noting the change in color of myocardial tissue in the ischemic area, and reperfusion was achieved by loosening the knot. The MI/RI rats were placed in different places for 24 hours of reperfusion, and then their physiological and biochemical indicators were tested.
| Geomagnetic shielding place | Geomagnetic radiation place | Normal place | |||
|---|---|---|---|---|---|
| Shield+sham group | Shield+operation group | Radiation+sham group | Radiation+operation group | Normal+sham group | Normal+operation group |

Myocardial Infarct Sizes
Following reperfusion, the heart was then excised, both atria and the right ventricle were removed, and the left ventricle was cut into five equal slices to create cross sections from apex to base. The slices were separated into normal zone and area at risk, both followed by incubation in 1% TTC to measure the viability of myocardial tissue. Viable tissue stained red, while nonviable tissue remained unstained or was white (Figure 2A). Infarct size as a percentage of area at risk was determined gravimetrically.


Left Ventricular Pressure Test
Cardiac function was measured by left ventricular cannulation. Rats were fasted for 12 hours and anesthetized with 3.6% chloral hydrate (1 ml/kg). The left common carotid artery was isolated, then the left ventricular developed pressure (LVDP), left ventricular end-diastolic pressure (LVEDP), and ± dP/dtmax were recorded by electrophysiolograph (BIOPAC 150).
Serum Biochemistry Test
The blood was collected from the abdominal aorta artery catheter and added to procoagulant tube to centrifuge for 3000 min at 4ºC. The serum was stored in an ultra-low temperature refrigerator at -20ºC. The automatic blood biochemical analyzer (Beckman AU480, USA) detect cTnI, CK, and LDH in the blood with specific reagents from AU Clinical Chemistry Systems.
Melatonin Test
The serum level of melatonin was detected by using the enzyme-linked immunosorbent assay (ELISA) kit according to the manufacturer’s instructions. The results were determined spectrophotometrically at 450 nm.
Statistical Analysis
All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) software, version 19 (SPSS Inc., Chicago, Illinois, USA). The data were presented as MEDIAN ± INTERQUARTILE RANGE and were compared using Kruskal-Wallis test. P<0.05 was considered statistically significant.
RESULTS
Myocardial Infarction Area
The results showed that there was no significant difference in the myocardial infarction area between the shielding + operation group, radiation + operation group, and normal+operation group (P>0.05), but there was significant difference in infarct size between the sham group and operation group (P<0.05) (Figure 2B).
Left Ventricular Pressure
The results showed that LVDP in the shield+operation group and normal+operation group were higher than in the radiation+operation group (P<0.05) (Figure 2C). There was no significant difference in LEVDP in the shielding+operation group and radiation+operation group (P>0.05), but in the shielding+operation group it was higher than in the normal+operation group (P<0.05) (Figure 2D). The ± dP/dtmax of the left ventricle in the shielding+operation group and normal+operation group were higher than that in the radiation+operation group(P<0.05) (Figure 2E).
Troponin I
The results showed that cTnI in the radiation+operation group was higher than in the shielding+operation group, and in the operation group it was higher than in the sham group (P<0.05) (Figure 3A).
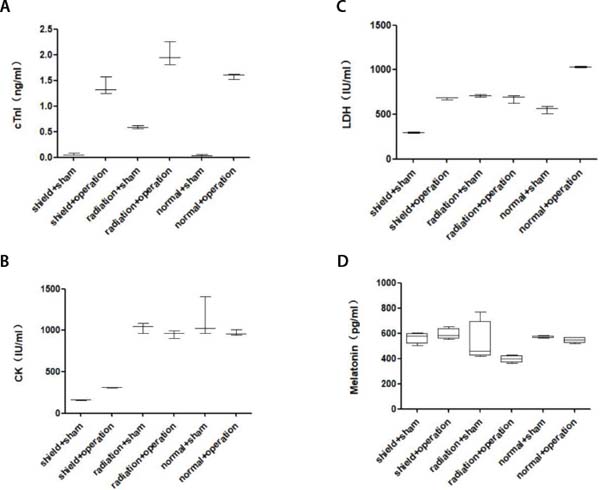

Creatine Kinase
The results showed that CK in the shielding+operation group was lower than in the radiation+operation group and normal+operation group (P<0.05) (Figure 3B).
Lactate Dehydrogenase
The results showed that LDH in the shielding+operation group had no significant difference from the radiation+operation group (P>0.05), but LDH in the shielding+operation group and radiation+operation group were lower than in the normal+operation group (P<0.05) (Figure 3C).
Melatonin
The concentrations of melatonin in the radiation+operation group were significantly lower than in the shielding+operation group and normal+operation group (P<0.05) (Figure 3D).
DISCUSSION
Among the many causes of MI/RI, humans began to notice the potential impact of geomagnetic activity on human health[6,7]. A vast number of large-scale clinical observational experiments show that when there was a geomagnetic outbreak, arrhythmia, hypertension, myocardial infarction, cerebral infarction, stroke, and other cardiovascular and cerebrovascular events increased significantly[3,9-12]. The mechanisms of the geomagnetic field on the cardiovascular function are studies that became very meaningful. Based on the discovered mechanism, we will prevent the geomagnetic effects and reduce the probability of cardiovascular diseases.
MI/RI lead to ventricular systolic and diastolic dysfunction[13,14]. From our experimental results, there was no significant difference on the myocardial infarction area between the shielding + operation group and radiation + operation group, but the LVDP and ± dP/dtmax in the radiation + operation group were lower than in the shielding + operation group and normal + operation group, and the LEVDP in the shielding + operation group was higher than in the normal + operation group, indicating that geomagnetic shielding can help to improve heart function and geomagnetic radiation can increase the damage in the heart function.
During MI/RI, myocardial oxygen free radicals accumulate, calcium overload occurs, and the myocardium produces a large amount of oxygen free radicals. These oxygen free radicals convert to hydroxyl free radicals, which act on the cell membrane and change the myocardial cell membrane structure and function. The cells release large amounts of LDH and CK, and they are specific indicators of myocardial injury[14,15]. From our experimental results, there are significant differences on CK between the shielding + operation group and radiation + operation group. This shows that geomagnetic activity has an impact on CK. We speculate that geomagnetic activity affects myocardial energy metabolism, muscle contraction, and adenosine triphosphate regeneration, because CK is correlated to those.
The cTnI is considered as the key biochemical marker in the diagnosis of myocardial injury. Patients with myocardial infarction have much higher concentrations of cTnI than healthy people[16]. From the experimental results, cTnI in the radiation + operation group is higher than in the shielding + operation group, indicating that geomagnetic radiation has an increasing effect on cTnI, while geomagnetic shielding has an inhibitory effect on cTnI, which proves that geomagnetic radiation has the potential to aggravate myocardial injury. Geomagnetic shielding has a protective effect on myocardial injury.
Melatonin has a powerful antioxidant effect and a high degree of diffusive penetration ability, which can exert its own antioxidant effect on the cell membrane, cytoplasm, and nucleus to protect the myocardial tissue against oxidative damage. From the experimental results, the concentration of melatonin in the radiation - operation group is lower than in the shielding + operation group and normal + operation group, indicating that geomagnetic radiation can reduce its protective effect on myocardial injury by inhibiting melatonin secretion. At the same time, the geomagnetic shield can promote the secretion of melatonin and enhance the protective effect of melatonin on myocardial injury[12,14,16].
CONCLUSION
The geomagnetic activity-related heat exposure is associated with an increase in cardiac events. This report describes the effect of geomagnetic outbreaks on the heart and how these outbreaks can aggravate damages from myocardial infarction. These findings identify the geomagnetic radiation damages to cardiovascular disease, which suggests that the impact of the space weather changing on human health cannot be ignored. In the view of the damage of geomagnetic outbreaks to the myocardium, we can predict the time of the geomagnetic outbreak in advance through early warnings from the astronomical observation, which may help to protect people from these outbreaks’ effects.
REFERENCES
1. Barquera S, Pedroza-Tobías A, Medina C, Hernández-Barrera L,Bibbins-Domingo K, Lozano R,et al. Global overview of the epidemiology ofatherosclerotic cardiovascular disease. Arch Med Res. 2015;46(5):328-38.doi:10.1016/j.arcmed.2015.06.006.
2. Feigin VL, Parmar PG, Barker-Collo S, Bennett DA, Anderson CS,Thrift AG, et al. Geomagnetic storms can trigger stroke evidence from 6 largepopulation-based studies in Europe and Australasia. Stroke. 2014;45(6):1639-45.doi:10.1161/STROKEAHA.113.004577.
3. Vencloviene J, Babarskiene R, Slapikas R, Sakalyte G. Theassociation between phenomena on the sun, geomagnetic activity, meteorologicalvariables, and cardiovascular characteristic of patients with myocardialinfarction. Int J Biometeorol. 2013;57(5):797-804.doi:10.1007/s00484-012-0609-8. [MedLine]
4. Yu L, Sun Y, Cheng L, Jin Z, Yang Y, Zhai M, et al. Melatoninreceptor-mediated protection against myocardial ischemia/reperfusion injury:role of SIRT1. J Pineal Res. 2014;57(2):228-38.doi:10.1111/jpi.12161.
5. Gao E, Lei YH, Shang X, Huang ZM, Zuo L, Boucher M, et al. A noveland efficient model of coronary artery ligation and myocardial infarction in themouse. Circ Res. 2010;107(12):1445-53.doi:10.1161/CIRCRESAHA.110.223925.
6. Berg H. [Solar and magnetic disturbances in relation to the medicometeorological prognoses]. Arch Phys Ther (Leipz). 1954;6(3):216-28.German.
7. Friedman H, Becker RO, Bachman CH. Geomagnetic parameters andpsychiatric hospital admissions. Nature. 1963;200:626-8.doi:10.1038/200626a0.
8. Mikulecký M, Strestík J. Cerebral infarction versus solar andgeomagnetic activity: a cross-regression study. Isr Med Assoc J.2007;9(12):835-8.
9. Simko F, Reiter RJ, Pechanova O, Paulis L. Experimental models ofmelatonin-deficient hypertension. Front Biosci (Landmark Ed). 2013;18:616-25.doi:10.2741/4125.
10. Lewczuk B, Redlarski G, Zak A, Ziólkowska N, Przybylska-Gornowicz B,Krawczuk M. Influence of electric, magnetic, and electromagnetic fields on thecircadian system: current stage of knowledge. Biomed Res Int. 2014;2014:169459.doi:10.1155/2014/169459.
11. Li JH, Yang P, Li AL, Wang Y, Shi ZX, Ke YN, et al. The preventiveeffect of garlicin on a porcine model of myocardial infarction reperfusionno-reflow. Chin J Integr Med. 2014;20(6):425-9.doi:10.1007/s11655-012-1091-1.
12. Soh S, Jun JH, Song JW, Shin EJ, Kwak YL, Shim JK. Ethyl pyruvateattenuates myocardial ischemia-reperfusion injury exacerbated by hyperglycemiavia retained inhibitory effect on HMGB1. Int J Cardiol. 2018;252:156-62.doi:10.1016/j.ijcard.2017.11.038. [MedLine]
13. Bartsch H, Mecke D, Probst H, Küpper H, Seebald E, Salewski L, etal. Search for seasonal rhythmicity of pineal melatonin production in rats underconstant laboratory conditions: spectral chronobiological analysis, and relationto solar and geomagnetic variables. Chronobiol Int. 2012;29(8):1048-61.doi:10.3109/07420528.2012.719958.
14. Burch JB, Reif JS, Yost MG. Geomagnetic activity and human melatoninmetabolite excretion. Neurosci Lett. 2008;438(1):76-9.doi:10.1016/j.neulet.2008.04.031.
15. Aimo A, Januzzi JL Jr, Vergaro G, Ripoli A, Latini R, Masson S, etal. Prognostic value of high-sensitivity troponin T in chronic heart failure: anindividual patient data meta-analysis. Circulation. 2018;137(3):286-97.doi:10.1161/CIRCULATIONAHA.117.031560. [MedLine]
16. Böhmer AE, Souza DG, Hansel G, Brum LM, Portela LV, Souza DO.Long-term cyclosporine treatment in non-transplanted rats and metabolic riskfactors of vascular diseases. Chem Biol Interat. 2010;185(1):53-8.doi:10.1016/j.cbi.2010.02.029.
Financial support: This study was funded by Research Institutes
in Yunnan Medical and Health Units Project, 2016NS075, and The
National Natural Science Foundation of China, 41764007.
No conflict of interest.
Authors’ roles & responsibilities
HW Substantial contributions to the conception or design of the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
WC The acquisition, analysis, or interpretation of data for the work; final approval of the version to be published
YD The acquisition, analysis, or interpretation of data for the work; final approval of the version to be published
XC The acquisition, analysis, or interpretation of data for the work; final approval of the version to be published
YD Final approval of the version to be published
XL Substantial contributions to the conception or design of the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
LD is responsible for the commissioning of geomagnetic experimental platform; final approval of the version to be published
Article receive on Friday, September 28, 2018
Article accepted on Tuesday, March 19, 2019
 All scientific articles published at rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at rbccv.org.br are licensed under a Creative Commons license



All rights reserved 2017 / © 2025 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()

 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket









